Background: Biventricular pacing has revolutionised the treatment of heart failure in patients with left bundle branch block; however, left ventricular-lead placement is not always technically possible. Direct left bundle pacing maybe a more physiological method of activating the heart and overcoming left bundle branch block. Therefore, this offers a promising alternative for cardiac resynchronisation when a coronary sinus (CS) left ventricular (LV) lead is unfeasible or has failed. We highlight a series of five cases where direct left bundle pacing was attempted when biventricular pacing failed.
Method: Direct left bundle pacing was attempted in five patients (four patients where CS LV lead was not possible and one patient with failed His bundle pacing). All of the procedures took place in a standard pacing lab. The Medtronic pacing system analyser was used for mapping with fluoroscopic guidance. The pre-shaped His sheath was used in all cases and after attempting to map a His signal the sheath was positioned high in the intra ventricular septum.
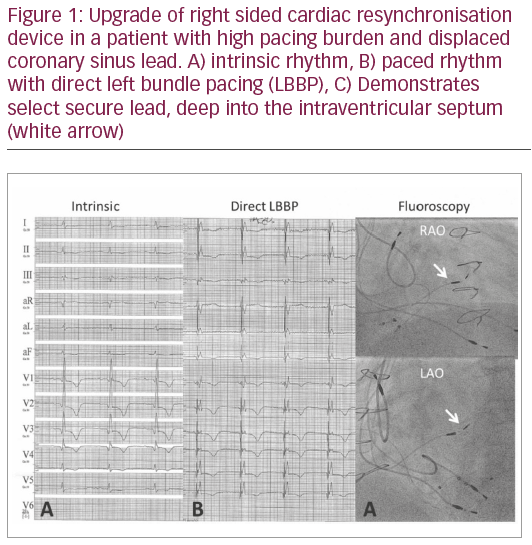
The select secure 3830 lead was deployed with multiple turns. Unipolar pacing was performed intermittently until narrowing of the QRS width and a qR pattern was seen in lead V1, indicating capture of the left bundle. All patients received a 1-month post-implant follow up as per department protocol.
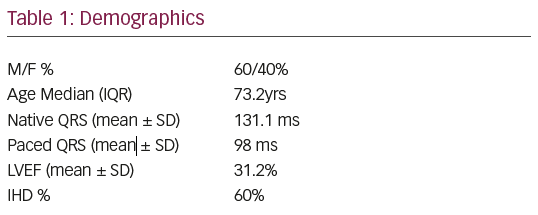
Results: Direct left bundle pacing was successful in four patients (Figure 1) and in one patient, non-selective his bundle pacing was accepted. The mean QRS decreased from 131.1 ms to 98.2 ms. The mean thresholds were 0.5 v @ 1.0 ms at the 1-month follow up. So far, two patients receive a 6-month follow up echo and LVEF has improved from 29% to 39%.
Conclusion: Direct left bundle pacing offers a potential alternative to cardiac resynchronisation therapy in patients where biventricular pacing is not possible using the coronary sinus. It is possible to achieve successful implantation without specialist electrophysiology equipment and pacing thresholds lower than with coronary sinus LV leads. Larger studies are needed to confirm the safety and long-term feasibility of this approach and whether it is applicable in other situations where right ventricular pacing is required.