Introduction: Ablation Index (AI) integrates catheter power, contact force and time to better inform operators about lesion delivery, and has shown promise in delivering more enduring pulmonary vein isolation. Many centres including our own routinely use contact force sensing to guide lesion delivery for atrial flutter ablation. One may encounter anatomical challenges when delivering lesions to the cavo-tricuspid isthmus (CTI) and we hypothesised that AI may provide valuable insight for more challenging cases. We investigated the relationship between AI values and impedance drop (ID) when delivering contact force guided ablation for typical atrial flutter.
Methods: We selected a random cohort of 20 patients (75% male, mean age 64.1 ± 13.1 years, median LVEF 42%) who underwent catheter ablation of typical atrial flutter in 2017-2018 using 3D electro-anatomical mapping and a contact force sensing catheter (CARTO, Biosense Webster). Visitag data was loaded into a CARTO unit with the AI algorithm installed and AI was calculated (Watts/grams/seconds – wgs) for 436 ablation lesions. The CTI lesions were anatomically bisected into ventricular and IVC ends of the ablation line. Procedural safety, clinical outcomes and associations between AI and ID were explored.
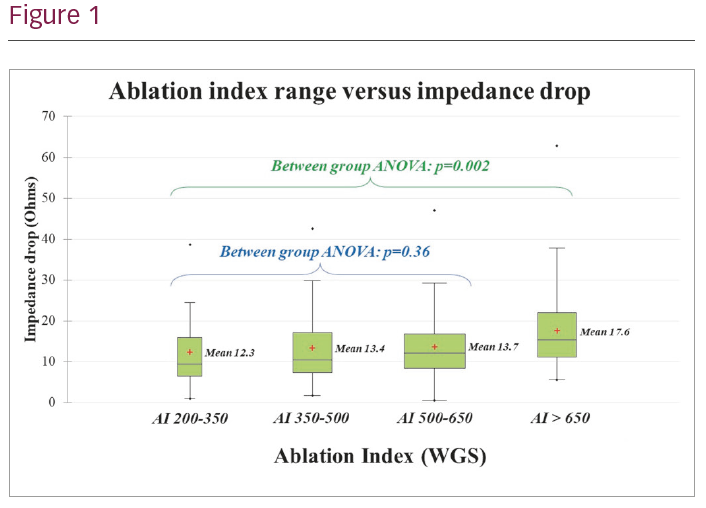
Results: There were no complications. Acute success (bidirectional block) was achieved in 100% of cases, but one recurrence of atrial flutter (5%) was seen during a mean follow-up of 6.6 ± 5.6 months. Mean AI for all lesions was 554 ± 133 wgs and mean ID 14.3 ± 8.9 Ohms; mean AI was similar between lesions at the ventricular and IVC margins (558 ± 131 wgs versus 548 ± 137 wgs, p=0.43) however mean ID was greater at the ventricular margin (15.4 ± 9.7 Ohms versus 13.3 ± 7.9 Ohms, p=0.014). There was no significant difference in mean ID between clusters of lesions delivered with an AI of 200–350 wgs (ID 12.3 ± 9.6 Ohms), 350–500 wgs (ID 13.4 ± 8.9 Ohms), or 500–650 wgs (ID 13.7 ± 8.2 Ohms, p=0.36). However, a significant increase in mean ID was seen in lesions where AI exceeded 650 wgs (ID 17.6 ± 9.5 Ohms, p=0.003), and mean AI was also found to be significantly higher in the one patient who suffered a recurrence (680 ± 120 wgs, p=0.0001).
Conclusion: Lesion ID cannot be used as a surrogate for the AI of a specific lesion when using contact force guided ablation for typical atrial flutter. These data may suggest we are currently ablating more than is necessary along the CTI. Prospective data with AI guided flutter ablation are needed to help inform physicians when deciding how much ablation is required during contact force guided flutter ablation.