Introduction: Biventricular pacing (BVP) improves morbidity and mortality in patients with heart failure and Left Bundle Branch Block (LBBB), but there is considerable scope for improved outcomes if more effective resynchronisation could be achieved. His bundle pacing (HBP) appears to be able to overcome LBBB and is a new method for Cardiac Resynchronisation Therapy (CRT). We performed an acute crossover comparison of HBP and BVP measuring effects on left ventricular activation time and pattern and acute haemodynamic function.
Methods: Twenty-four patients with LBBB referred for a BVP device implantation based on standard clinical criteria were recruited. Using high precision, beat-by-beat assessment of acute systolic blood pressure, we compared haemodynamic responses to BVP and temporary HBP. We used ECGI to measure left ventricular activation time (LVAT) and to perform epicardial propagation mapping (EPM) allowing visualisation of activation patterns. Eleven patients with normal, narrow QRS undergoing ECGI recordings were analysed for comparison.
Results: In 17 patients, temporary HBP reduced activation time (termed ‘His-CRT’) and the full haemodynamic and ventricular activation dataset was successfully acquired. His-CRT was more effective in delivering ventricular resynchronisation than BVP; it delivered significantly greater reductions in QRS duration (–18.6 ms, 95% CI –31.6 to –5.7, p=0.007) and LVAT (–26 ms 95% CI –41 to –21, p=0.002). This translated into a significantly greater acute systolic blood pressure response (4.6 mmHg, 95% CI 0.2 to 9.1, p=0.04). Changes in activation time showed a close correlation with changes in acute systolic blood pressure (R=0.7, p=0.04).
EPM revealed two distinct activation patterns in LBBB. In the majority of patients (20/24, 83.3%), regions of epicardial propagation block were observed. In the remainder of patients with LBBB (4/24, 16.7%), a second pattern was observed: slow propagation across the LV epicardium without any appearance of blocked or regionally slowed conduction.
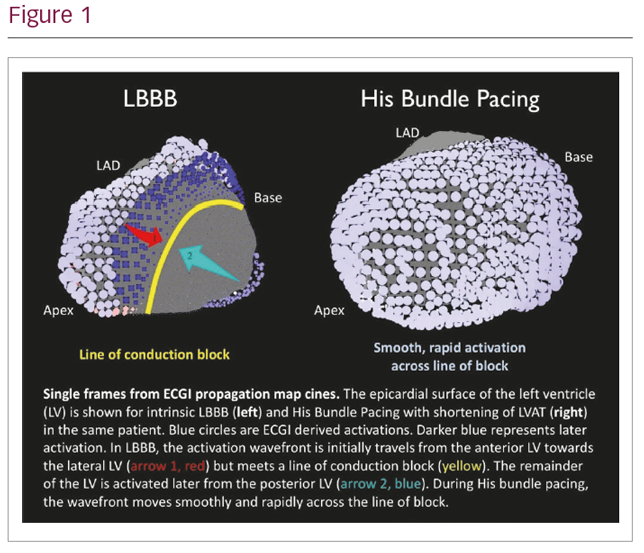
In patients where His-CRT produced LVAT-95 values within the normal range defined by participants with normal, narrow QRS (24–70 ms), lines of block disappeared with HBP which produces smooth, rapid activation of the LV indistinguishable from activation pattern in patients with normal QRS (Figure 1). In patients without lines of block, LVAT was not reduced by HBP. Regression modelling demonstrated that propagation block predicted LVAT-95 shortening (p=0.04).
Conclusions: EPM derived from ECGI allows accurate non-invasive discrimination of LBBB with regions of propagation block, that is potentially amenable to resynchronisation by HBP, from diffuse slow conduction that cannot be corrected. When HBP normalises left ventricular activation time, the activation pattern produced is physiological and indistinguishable from normal activation with intact conduction system. This translates to improved haemodynamic function compared to BVP.