Background: Accurately determining arrhythmia mechanism from a 12-lead ECG of supraventricular tachycardia (SVT) can be challenging. Machine learning, with convolutional neural networks (CNNs) in particular, has been used to classify arrhythmias using the 12-lead ECG with great accuracy. However, most studies use human interpretation of the ECG as the ground truth to label the arrhythmia ECGs. Therefore, these neural networks can only ever be as good as expert human interpretation. We hypothesised a convolutional neural network can be trained to classify atrioventricular re-entrant tachycardia (AVRT) vs atrioventricular nodal re-entrant tachycardia (AVNRT) from the 12-lead ECG, when using findings from the invasive electrophysiology (EP) study as the gold standard.
Methods: We trained a CNN on data from 124 patients undergoing EP studies with a final diagnosis of AVRT or AVNRT. A total of 4962 5-second 12-lead ECG segments were used for training. Each case was labelled AVRT or AVNRT based on the findings of the EP study. The model performance was evaluated against a hold-out test set of 31 patients.
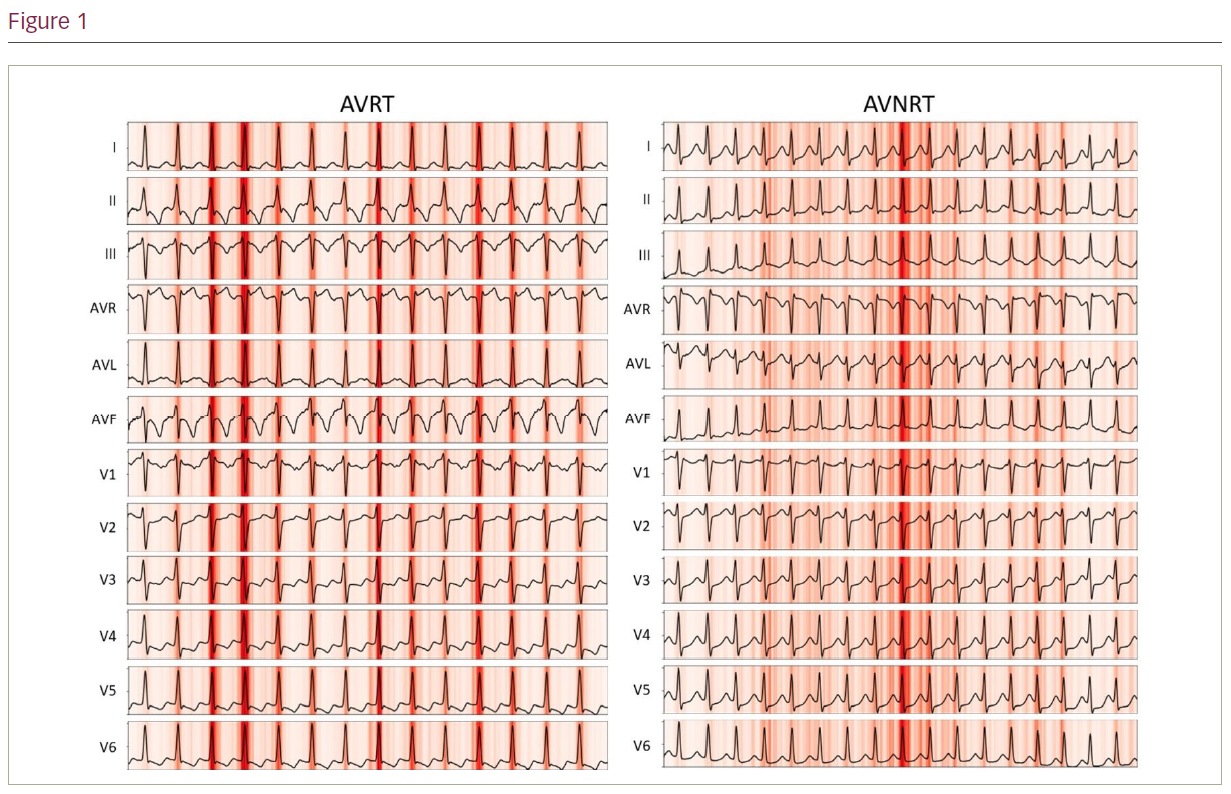
Results: The model had an accuracy of 77% in distinguishing between AVRT and AVNRT. The area under the receiver operating characteristic curve was 0.80. A saliency map can be used to help understand why a CNN predicted a particular outcome. This is achieved by mapping the outcome back to key areas of the input that most influenced the network in producing the classification result. Figure 1 presents the saliency mappings of an example 12-lead ECG for each class of AVRT and AVNRT. The network used the expected sections of the ECGs for diagnoses; these were the QRS complexes which may contain retrograde p waves.
Conclusion: We describe the first neural network trained to differentiate AVRT from AVNRT. Our model achieved a reasonable accuracy and demonstrated proof-of-concept. Accurate diagnosis of AVNRT from a 12-lead ECG could allow for empirical slow pathway ablation in cases where dual atrioventricular nodal physiology is present but sustained arrhythmia cannot be induced during the EP study. The current accuracy from our neural network does not yet meet this threshold, but may be improved with a larger training dataset. ❑