Introduction: Cardiac resynchronisation therapy (CRT) is a routine treatment for heart failure with reduced ejection fraction with conduction delay to improve symptoms and prognosis in patients. Technological advancements both in imaging cardiovascular magnetic resonance (CMR) and devices (sophisticated MRI-conditional modes) enable investigation of the haemodynamic response to CRT over a range of heart rates.
Methods: Patients with a CRT-D device were enrolled from heart failure clinics at Leeds General Infirmary, Leeds. After an MRI safety assessment, a baseline device interrogation was conducted by a cardiac physiologist. Left ventricular (LV) volumes and systolic blood pressure were measured at baseline and heart rates of 75, 90, 100, 115, 125 and 140 (randomised order) with CRT active and intrinsic/RV conduction. All scans were conducted using a 3.0 T Siemens Prisma human MRI scanner. Analysis of the scans used commercially available software (cmr42, Circle Cardiovascular Imaging Inc, Calgary, AB, Canada) and manual contouring was completed for LV systole and diastole at each heart rate. A post-scan device interrogation was conducted to assess for scanning safety.
Results: In this randomised crossover study, scanning was conducted in 17 patients (Table 1) across the range of heart rates with CRT active and disabled. Post-scan battery voltage from baseline was –2.92 and 2.90% (p=ns) with CRT active and disabled respectively. Overall lead impedance change was –0.1% and 0.91% (p=ns) in patients with CRT active and disabled respectively. No statistical difference was found between CRT modes, furthermore, no patient experienced symptoms related to scanning or device failure.
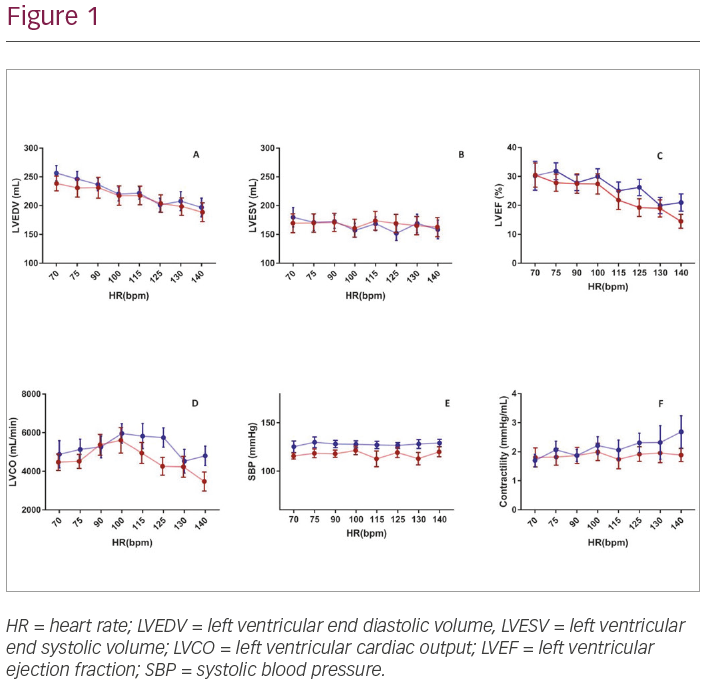
Contractility increases across heart rates when CRT is active whilst relatively static when CRT is disabled. At the peak heart rate of 140 bpm, mean contractility was 2.6 mmHg/mL compared with 1.98 mmHg/mL (p=0.05) when CRT was active and disabled respectively. Other heart rates failed to reach statistical significance in terms of contractility when alternating CRT modes.
LVEF is reducing with increased atrial pacing in keeping with cardiac physiology. Mean LVEF was 26.2% versus 19.3% (p<0.01) when CRT was active and disabled respectively. Furthermore, at 140 bpm LVEF was 19.3% versus 13.3% (p<0.01) with CRT active and disabled respectively.
LVCO appears to have a bell-shaped curve across heart rates in heart failure patients which widens when CRT is active. Mean LVCO at 125 bpm was 5,749 mL/min versus 4,254 mL/min (p<0.01) with CRT active and disabled respectively. Similarly, at 140 bpm LVCO was 4,994 mL/min versus 3,241 mL/min (p=0.02) with CRT active and disabled respectively.
Mean SBP across the HR range was 127.8 mmHg versus 117.5 mmHg (p<0.0001) whilst CRT was active and disabled respectively.
Conclusion: We have demonstrated for the first time, the mechanistic improvements in cardiac contractility consequent to CRT using CMR and the relative safety of this approach. Furthermore, varying atrial pacing rates appear to have unique effects on cardiac response patients suggesting tailored programming may benefit this cohort.