Introduction: It is widely accepted that the methods for optimising CRT vary in clinical practice. Electrical optimisation of CRT is becoming more popular with QRS narrowing and favourable ECG characteristics emerging as markers of success (1). The aim of this survey was to gauge current working practices of CRT within the UK and Ireland, with particular emphasis on the ECG.
Method: Voluntary completion of a short online questionnaire (8 questions) via Survey Monkey. This was circulated widely on two key social media platforms (Facebook & Twitter) and aimed at Cardiac Physiologists & Cardiology Clinicians. The survey remained open between 28/04/2020 and 15/05/2020.
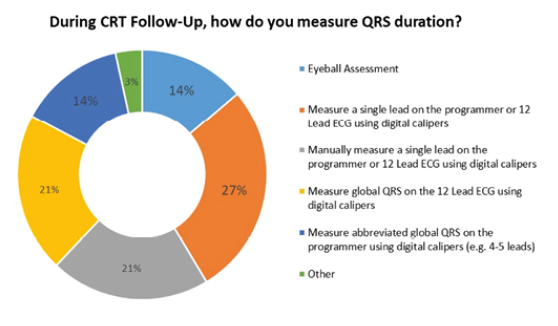
Results: There were 31 responses representing 20 CRT centres within the UK and Ireland with wide geographical spread. 97% agreed that QRS narrowing was important in CRT. 84% measured QRS duration on implant, but only 55% measured QRS duration routinely at follow up. The type of ECG monitoring during CRT Implant varied between centres; 48% used 12 Lead ECG; 29% used limbs leads plus 1-2 chest leads and 19% used limb leads only. There was also variation in the type of ECG monitoring during CRT follow-up; 42% routinely used programmer ECG plus 12 Lead ECG; 16% used 12 Lead ECG only; 16% used programmer ECG only; 26% used programmer ECG with the addition of 12 Lead ECG on an individual basis. Measurement technique for QRS duration varied on implant; 35% measured a single ECG lead using digital calipers; 10% manually measured a single ECG lead; 35% measured global QRS on the 12 Lead ECG using digital calipers; 13% measured abbreviated global QRS on the programmer using digital calipers (e.g. 4-5 leads); 3% used eyeball assessment and 3% did not measure QRS duration. Similar variation in the measurement of QRS duration was noted during follow-up (see graph).
Discussion: The results highlight wide variation in practice across the UK and Ireland. The optimal electrical characteristics of CRT are best assessed using 12 Lead ECG but this is not universally accepted in clinical practice. QRS duration is considered important during CRT, but there is inconsistency in both the type of ECG monitoring and the methods used to assess QRS narrowing in both implant and follow-up. Studies have shown that QRS duration can vary depending on the measurement technique, with global QRS considered superior to single lead measurement. CRT Optimisation clinics are growing in popularity and it may be beneficial to standardise the type of ECG assessment and also the measurement of QRS duration to ensure quality and consistency.
References:
- Sweeney MO, Hellcamp AS, van Bommel RJ, et al. QRS fusion complex analysis using wave interference to predict reverse remodelling during cardiac resynchronisation therapy. Heart Rhythm. 2014;11:806–816.
Figure: