There are several beneficial effects of statins on the progression of atherosclerosis, and there have been significant advancements in pharmacotherapies for atherosclerotic cardiovascular disease (ASCVD). However, substantial residual cardiovascular (CV) risk remains, and there is an unmet need to reduce the residual risk of cardiovascular disease (CVD) events.1 There is increased focus on the role of atherogenic dyslipidaemia, particularly elevated triglycerides (TGL), as important mediators of residual risk, which is highlighted in epidemiologic and genetic/Mendelian randomisation studies and supports the hypothesis of elevated TGLs as a suitable therapeutic target.2–4 Clinical studies have shown that omega 3 fatty acids (OM3FA) are effective in lowering TGLs; however, to date, trials and meta-analyses of combined OM3FA products have not demonstrated any clinical CV outcome benefit in patients receiving statins.5 Icosapent ethyl (IPE), a highly purified, stable ethyl ester of eicosapentaenoic acid (EPA), has emerged as a useful adjunctive therapy to address residual CV risk in recent trials.6–9 In this brief review, we will provide an overview of the mode of action of IPE in coronary atherosclerosis, the robust clinical evidence and trial data supporting its use, and expert consensus/recommendations on its use in specific populations, as an adjunct to existing anti-atherosclerotic therapies.
Insights from trials of omega 3 fatty acid preparations
Based on epidemiological associations between OM3FAs and reduced CV morbidity and mortality in populations with CV risk, numerous randomised clinical trials have studied the benefit of OM3FAs on clinical outcomes.10,11 As we explore the evolution of OM3FA in CV clinical trials, we note that most earlier studies in OM3FAs included dietary supplements or heterogeneous preparations of combinations of docosahexaenoic acid (DHA) and EPA, and have failed to show significant improvement in CV risk and incidence of CV events (Table 1).12–27
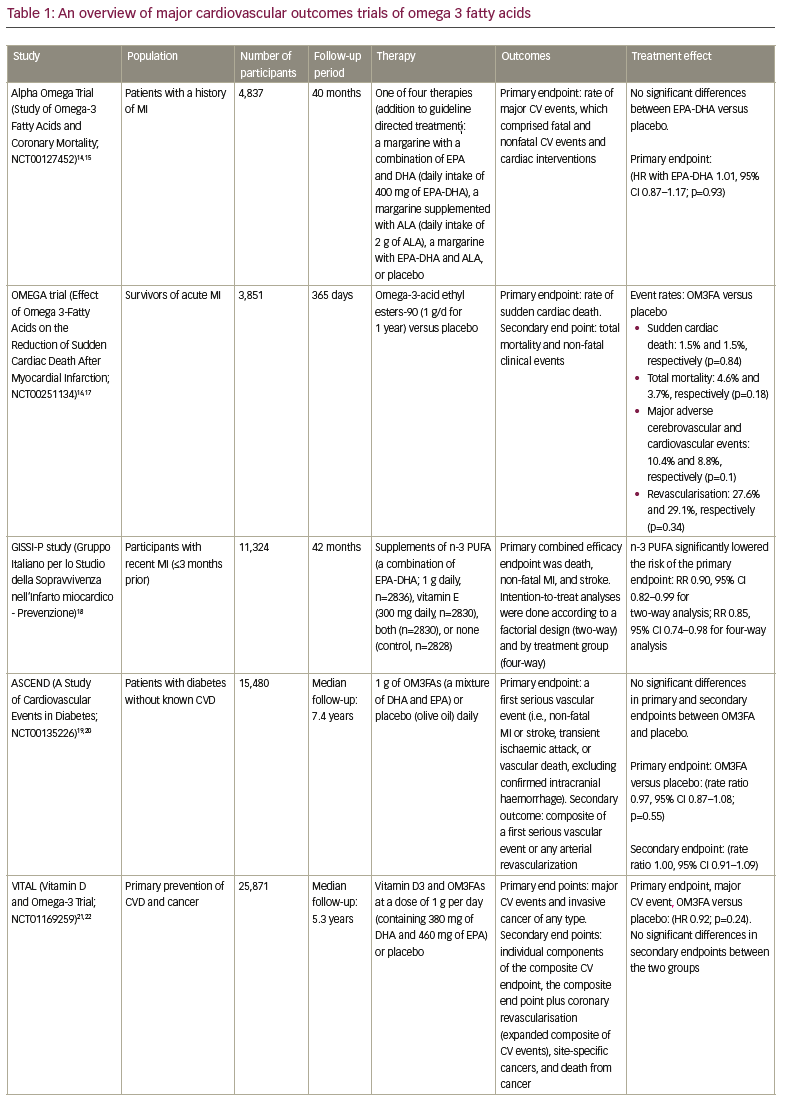
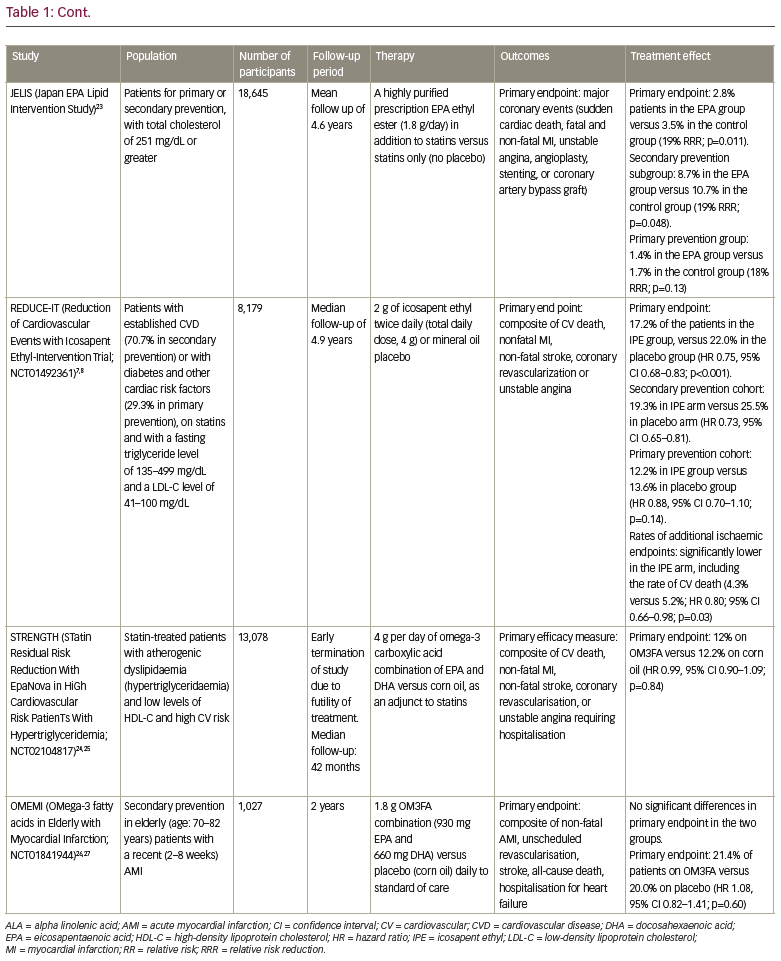
The initial trials of OM3FA included dietary supplements, as in the Alpha Omega trial (ClinicalTrials.gov identifier: NCT00127452; 400 mg per day of EPA-DHA) and the OMEGA trial (ClinicalTrials.gov identifier: NCT00251134; 1g per day of EPA-DHA), where low-dose supplementation with EPA-DHA failed to demonstrate significant reductions in CV events in high-risk patients with a history of myocardial infarction (MI).14-17 The ASCEND study (A Study of CV Events in Diabetes; ClinicalTrials.gov identifier: NCT00135226) compared the effect of 1 g of OM3FAs (a mixture of DHA and EPA) or placebo (olive oil) on CV outcomes, in a high-risk population with diabetes with no known history of CVD (primary prevention).19,20 After a mean follow-up of 7.4 years, there was no significant difference in the risk of serious vascular events between the two groups (8.9% of patients in treatment group versus 9.2% in the placebo group, rate ratio 0.97, 95% confidence interval [CI] 0.87–1.08).19,20 In another primary prevention trial of CVD, the Vitamin D and Omega-3 Trial (VITAL; ClinicalTrials.gov identifier: NCT01169259) randomised 25,871 participants in a two-by-two factorial design, and reported no significant reduction in the rate of major CV events in the treatment group who received vitamin D3/OM3FAs at a dose of 1 g per day (containing 380 mg of DHA and 460 mg of EPA; hazard ratio [HR] 0.92, 95% CI 0.80–1.06).21,22 Most recently, the STatin Residual Risk Reduction With EpaNova in HiGh Cardiovascular Risk PatienTs With Hypertriglyceridemia (STRENGTH) trial (ClinicalTrials.gov identifier: NCT02104817) randomised 13,078 participants and compared a mixture of EPA and DHA with corn oil in statin-treated participants with high CVD risk, hypertriglyceridaemia, and low levels of high-density lipoprotein cholesterol (HDL-C).24,25 The trial failed to demonstrate significant CV benefit and was terminated early for futility. Furthermore, the OMega-3 fatty acids in Elderly with Myocardial Infarction (OMEMI; ClinicalTrials.gov identifier: NCT01841944) trial evaluated the effects of adding 1.8 g OM3FA (a combination of 930 mg EPA and 660 mg DHA) versus placebo (corn oil) daily to standard-of-care treatment in a vulnerable cohort of elderly patients with a recent (2–8 weeks) acute MI.26,27 There was no reduction in clinical events in the elderly patients treated with OM3FA for 2 years (primary endpoint: 21.4% on OM3FA versus 20% on placebo; HR 1.08, 95% CI 0.82–1.41; p=0.60).
The clinical benefits of EPA were highlighted in JELIS (Japan EPA Lipid Intervention Study), an open label, randomised trial where 18,645 statin-treated participants (primary prevention cohort of 14,981 participants and secondary prevention cohort included 3,664 participants) were randomised to treatment with 1.8 g/day EPA ethyl ester, a highly purified OM3FA, or statin alone (no placebo).23 Unlike previous OM3FA trials, which used combinations of EPA-DHA, JELIS examined the effectiveness of a highly purified prescription EPA ethyl ester, as an adjunct to statins. Significant reduction in ASCVD events were observed in the EPA treatment group (HR 0.81, 95% CI 0.69–0.95; p=0.011), with consistent benefits across primary and secondary prevention cohorts. The differential trial results of heterogeneous OM3FA combinations and purified EPA preparations bring to our attention important insights with respect to the composition and purity of OM3FAs and dosage levels of EPA, which were incorporated in REDUCE-IT.
The Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial
The Reduction of Cardiovascular Events with Icosapent Ethyl-Intervention Trial (REDUCE-IT) was a randomised, double-blinded, placebo-controlled trial and sought to evaluate if treatment with 4 g/day of IPE (a highly purified ethyl ester of EPA), as an adjunct to statins would lower the incidence of ischaemic events in vulnerable patients at risk for ASCVD (primary and secondary prevention) and residually elevated fasting TGL (135–499 mg/dL).28
Randomised participants in the primary prevention stratum (29.3%) were required to be ≥50 years of age, with diabetes mellitus and at least one additional CV risk factor; and those in the secondary prevention stratum were required to be ≥45 years of age and with established CV disease. REDUCE-IT investigators randomised 8,179 participants to receive 4 g per day of IPE, compared with a mineral oil placebo. In a landmark outcome, treatments with IPE reduced the incidence of ischaemic CV events by 25% (HR 0.75, 95% CI 0.68–0.83; p=0.00000001), when compared with placebo.7 Furthermore, when stratified by risk category, both primary (HR 0.81, 95% CI 0.62–1.06) and secondary (HR 0.71, 95% CI 0.63–0.82) prevention cohorts demonstrated meaningful reductions in the incidence of primary and secondary endpoints. A follow-up analysis demonstrated a consistent and significant benefit of reduction in event burden with IPE, when the totality of subsequent ischaemic events were incorporated (HR 0.70, 95% CI 0.62–0.78; p=0.00000000036).29 A subgroup analysis of high-risk patients with diabetes revealed robust clinical benefits, irrespective of patients’ history of CVD at baseline.30 In terms of benefits with rates of revascularization, IPE further lowered the need for first and subsequent coronary revascularizations, including both percutaneous coronary intervention (PCI) and coronary artery bypass grafting.31 These findings from REDUCE-IT underscore the sharp contrast in results from previous outcome trials of heterogeneous OM3FA preparations, and highlight the robust benefits and generalisability of IPE in a broad population of at-risk patients.32 The mounting evidence in support of IPE leads us to understand the unique mechanisms of action of EPA, the significance of dosage, purity and composition of OM3FA preparations, and its distinct effects on coronary atherosclerosis.
Mechanisms of action: Icosapent ethyl pleiotropy
Although REDUCE-IT was designed to recruit participants with persistently elevated TGL, the results across subgroups suggest that at least some of the effects of IPE on the incidence of CV events may be mediated by effects beyond the reduction of TGL and lipoproteins.6 First, the degree of benefit observed with treatment by IPE was similar and significant across all tertiles of baseline and attained/on-treatment TGL levels. Second, the magnitude of observed benefit of 25% relative risk reduction for the primary composite endpoint cannot be correlated with the magnitude of differences in TGL levels between the treatment arms.9 These data from REDUCE-IT and emerging evidence from numerous studies suggest a myriad of beneficial effects of EPA that contribute to CV risk reduction beyond the effects on lipid biomarkers and TGL levels.
Studies suggest unique beneficial effects of IPE that include a wide spectrum of downstream effects on cell membrane stabilisation, improved endothelial function, lipid oxidation, and anti-thrombotic and anti-inflammatory properties.33 These mechanisms attest to the drug’s categorisation as being potentially pleiotropic. Emerging evidence continues to validate the biologic plausibility of actions of EPA as an anti-atherosclerotic agent, with effects along the pathophysiological cascade of coronary atherosclerosis, from initiation of plaque formation to plaque progression, stability and rupture.34 The Effect of Vascepa on Progression of Coronary Atherosclerosis in Persons With Elevated Triglycerides on Statin Therapy (EVAPORATE) trial (ClinicalTrials.gov identifier: NCT02926027) sought to understand the mechanistic effects of IPE as an adjunct to statins on coronary plaque characteristics and volumes by serial coronary computed tomography angiography (CCTA), in a population with CVD with persistently high TGLs, similar to REDUCE-IT.35,36 IPE demonstrated slowed rates of progression of most coronary plaque types at 9 months, with sustained and significant benefits at 18 months, including regression of high-risk plaque characteristics/low attenuated plaque volume, compared with placebo.37,38 In a follow-up analysis, IPE, when added to statin therapy, was associated with increased fibrous cap thickness at 9 months, suggesting reduction in vulnerable plaque features, leading to a more stable plaque phenotype.39 Similarly, the Combination therapy of eicosapentaenoic acid and pitavastatin for coronary plaque regression evaluated by integrated backscatter intravascular ultrasonography (CHERRY) trial investigated the effects of EPA/pitavastatin (PTV) (EPA 1,800 mg/day and PTV 4 mg/day) versus PTV only, on coronary plaque progression and stability features analysed by integrated backscatter intravascular ultrasound, in patients with known CVD who had undergone recent PCI.40 They demonstrated significantly reduced coronary plaque volumes and increased plaque stabilisation in combination EPA/PTV therapy versus statins alone.
In addition to lowering TGL, the beneficial effects of IPE on lipoprotein loading in the initial steps of atherogenesis are significant. Treatment with IPE is shown to lower circulating atherogenic lipoproteins, including apoB, and lipoprotein-associated phospholipase A2, highlighting its anti-oxidant properties.41,42 Atherosclerosis has been identified as a chronic inflammatory condition, with maladaptive immune-inflammatory responses being described as the key pathophysiologic mechanism contributing to initiation, propagation and progression of atherosclerosis.43 A favourable impact on markers of inflammation has been demonstrated in clinical studies; the Effect of AMR101 (Ethyl Icosapentate) on Triglyceride (Tg) Levels in Patients on Statins With High Tg Levels (≥200 and <500 mg/dL) (ANCHOR) and Efficacy and Safety of AMR101 (Ethyl Icosapentate) in Patients With Fasting Triglyceride (Tg) Levels ≥500 and ≤2000 mg/dL (MARINE) trials showed that EPA significantly reduced high-sensitivity C-reactive protein (hsCRP) in participants with residually elevated TGL and in a sub-analysis of patients with metabolic syndrome.44–47 In summary, the role of EPA in reducing the circulating load of major atherogenic lipoproteins beyond TGL, along with concomitant anti-oxidant and anti-inflammatory activity, regulates the cascade of atherosclerosis, which likely leads to a profound impact on adverse CV outcomes.
Distinct mechanistic effects of eicosapentaenoic acid versus docosahexaenoic acid
The differential and distinct mechanisms of action of EPA and DHA on factors related to coronary atherogenesis, may explain the differences in results of outcome trials of OM3FA preparations, such as REDUCE-IT and STRENGTH. In a pre-specified analysis of REDUCE-IT, the degree of, and time to, CV benefit from IPE was closely related to the serum EPA levels achieved, with a 37% relative risk reduction observed in the highest EPA tertile, which was 2.5-fold greater than in the lowest tertile (p<0.0001).48 The magnitude of CV benefits in REDUCE-IT is likely strongly correlated with on-treatment serum EPA levels via IPE, compared with changes in CV biomarkers such as low-density lipoprotein cholesterol (LDL-C) or hsCRP. A potential explanation for the robust CV benefits in REDUCE-IT can be linked to the higher dosage of EPA and the specific formulation of IPE, which has not been studied in prior trials, including those with combination mixtures of EPA-DHA. In a sub-analysis of the EVAPORATE trial, higher serum EPA levels were shown to predict regression of prognostically relevant coronary plaque volumes, total non-calcified plaque, and total plaque on CCTA.49 These results build on existing evidence to strongly suggest EPA levels act as a key mediator to mechanisms of benefit with IPE.48
There is increasing evidence to demonstrate the distinct effects of EPA and DHA on coronary atherosclerotic pathways through the differential influence on membrane structure, oxidation of lipids, inflammation and endothelial function.33 The favourable molecular structure and lipophilic nature of EPA, in contrast to DHA, contributes to the increase in membrane stability, improved lipoprotein clearance and reduced inflammation.50 However, studies indicate that DHA influences membrane fluidity and structure in a non-uniform manner, and promotes the formation of cholesterol-rich domains that are pro-atherogenic and promote the formation of unstable atherosclerotic plaques.51 EPA also exhibits important anti-oxidant properties that are not reproduced with DHA even under hyperglycaemic states.52 EPA and DHA are known to have different effects on the LDL receptor, as DHA may reduce LDL receptor expression and LDL particle clearance, while EPA enhances the clearance of LDL particles. Most importantly, the anti-inflammatory effect of EPA has been demonstrated in clinical trials with significant reductions in serum inflammatory biomarkers, which has not been consistently demonstrated in trials with EPA/DHA mixtures.33,53 In MARINE and ANCHOR, IPE significantly decreased TGLs without raising LDL-C, unlike DHA, which can increase LDL levels.54 Imaging trials further allude to the differential effects of pure EPA preparations on coronary atherosclerosis versus EPA/DHA combinations. The CHERRY and EVAPORATE trials highlight the early and substantial effects of EPA on the reduction of atherothrombotic burden, demonstrated by a reduction of coronary plaque volumes in the EPA group compared to placebo. In contrast, no significant differences in coronary plaque progression were observed when comparing statin-treated subjects with stable coronary artery disease, who received OM3FA (1.86 g of eicosapentaenoic acid and 1.5 g of docosahexaenoic acid daily) versus no omega-3 (control) for 30 months.55
Beyond the unique effects of EPA and DHA on several factors related to coronary atherogenesis, the inconsistencies in observed benefits related to EPA alone versus combination of EPA plus DHA, remains to be completely understood. Mechanistic studies are needed to explore if the addition of DHA may diminish or negate the beneficial properties of EPA, which could explain some of the discordant results observed in the REDUCE-IT and STRENGTH trials.
There has been some interest in the effect of different placebos used in the REDUCE-IT trial (mineral oil) versus the STRENGTH trial (corn oil) on the differential outcomes of the trials. Concerns have been raised regarding the validity of results in the REDUCE-IT trial, in part questioning the stipulated biological activity of the mineral oil placebo linked to observed changes in cardiac biomarkers in the placebo arm of the trial. In a post-hoc analysis comparing serial CCTA in the mineral oil placebo arm in EVAPORATE to a cellulose-based placebo cohort in the GARLIC5 study, no differences were observed in the rate of coronary plaque progression in the two groups.56,57 In addition, consistent and significant benefits of EPA on coronary atherosclerosis and CV outcomes have been demonstrated in Japanese populations in the open-label CHERRY and JELIS trials, where no placebo comparator groups were included.40,58
A detailed review of literature has shown that mineral-oil-related changes in TGL, low-density lipoprotein cholesterol and other biomarkers have been mostly inconsistent across studies, and are not clinically meaningful to explain the substantially positive results of REDUCE-IT.59 In a review of REDUCE-IT by the US Food and Drug Administration (FDA), they concluded that the magnitude of difference in outcomes between IPE and mineral oil groups could not be explained by the stipulated harmful effects of mineral oil placebo.60 Therefore, a summary of current evidence supports the validity of CV benefits with IPE in the REDUCE-IT and EVAPORATE trials, and attests to the results not being influenced by the small amount of mineral oil used in the placebo capsules.
Clinical implications
IPE has received support from leading medical bodies across the world for its robust clinical efficacy, well-established safety profile and cost effectiveness, making it an important addition to address residual CV risk.61
Currently, IPE is the first and only available medication approved by the FDA, ‘to be used as an adjunct to maximally tolerated statin therapy to reduce the risk of myocardial infarction, stroke, coronary revascularisation, and unstable angina requiring hospitalisation in adult patients with elevated TG levels (≥150 mg/dL [1.69 mmol/L]) and established CV disease or diabetes mellitus and two or more additional risk factors for CV disease’.62 Based on the findings from REDUCE-IT, the European Society of Cardiology guidelines recommend the use of IPE for residually elevated TGL levels, despite statins (class IIa, level B recommendation). The American Diabetes Association’s 2020 ‘Standards of Medical Care in Diabetes’ and the National Lipid Association recommend the addition of IPE as an adjunct to statins to lower residually elevated TGL in primary prevention cohorts/high-risk patients with diabetes and ≥1 additional CV risk factor.63,64
Adverse effects
In the REDUCE-IT population, the overall rates of adverse events during the trial or the rates of serious events associated with discontinuation of treatment (drug or placebo) were comparable between the two groups. Participants in the treatment group had higher rates of new onset atrial fibrillation in the IPE arm compared with the placebo group (5.3% versus 3.9%), and a relatively higher incidence of hospitalisations for atrial fibrillation or flutter (3.1% versus 2.1%, p=0.004). Given the physiological anti-thrombotic and antiplatelet effects of OM3FA/EPA, bleeding rates were closely monitored in the trial. The rates of serious bleeding events were more frequent in the treatment group, 2.7% versus 2.1% (p=0.06), with no reports of fatal bleeding events in both groups.7 There were no significant differences between IPE and placebo in rates of adjudicated haemorrhagic stroke (0.3% versus 0.2%, p=0.55) or gastrointestinal bleeding (1.5% versus 1.1%, p=0.15) in the two groups.
Importantly, the overall safety profile of 4 g per day of IPE has been well documented with no change in benefit/risk assessments of the trial, when rates of atrial fibrillation and/or serious bleeding events were incorporated into the endpoint ascertainments in post-hoc analyses.65
Expanding the indications for future use of icosapent ethyl
The substantial, consistent and clinically meaningful results across CV endpoints and subgroups (primary and secondary prevention cohorts) in REDUCE-IT has fuelled tremendous interest in extrapolating the application and clinical utility of IPE to additional high-risk patient subgroups, beyond the patients included in current guidelines. Remarkably, the clinical benefits of IPE that were observed in REDUCE-IT were independent of baseline or attained TGL levels.66 It is also important to highlight that 10% of the participants included in REDUCE-IT had normal TGL levels, and their relative risk reductions were comparable to patients with higher TGL levels.9,67 These data further suggest that the CV risk reductions observed with IPE were largely related to changes in serum EPA levels and its associated pleiotropic effects, and not mere changes in lipid biomarker or TGL levels. Multiple registry and cost-effectiveness analyses have identified a large proportion of patients at higher risk of CVD who could potentially benefit from IPE and the application of REDUCE-IT results, irrespective of serum TGL levels.32,68,69 Another important subgroup of participants that could be considered for the potential expanded role of IPE may be high-risk patients with known coronary atherosclerosis or diabetes mellitus with normal TGL levels. Another subset who may benefit from IPE beyond the current guideline recommendations may include patients who are intolerant to statins (representing nearly 4 million adults in the USA) with elevated TGL ≥150 mg/dL and high CV risk.
In summary, IPE offers an exciting therapeutic option to the multitude of anti-atherosclerotic and preventive therapies that are emerging, and can contribute to an improvement in CV outcomes across a spectrum of CV risk. Future studies must continue to examine and elucidate the myriad of plausible mechanisms of action of IPE in coronary atherosclerosis, and explore its beneficial applications and use in wider populations.