Introduction: Recurrence of persistent atrial fibrillation (PsAF) has been attributed to conduction gaps, and non-transmural linear lesion sets. Hybrid thorascopic endo-epicardial AF ablation has been shown to reduce AF recurrence when compared to endocardial ablation alone, however with higher complication rates. We propose that the percutaneous pericardial CO2 insufflation technique to access the pericardial space can be safely and effectively used for epicardial mapping and ablation of the left atrium (LA).
Methods: In a single centre, 11 patients with PsAF and previous pulmonary vein isolation (PVI) only, underwent concurrent endo-epicardial AF ablation, using the subxiphoid percutaneous pericardial access technique using CO2 insufflation of the pericardial space, whilst on uninterrupted anticoagulation. Heparinisation targeted an activated clotting time of 350 s. Endo-epicardial geometry and bipolar voltage maps were created, and endocardial ablation performed. The target LSI was 5 for the inferior line, and 6 on the roof and anterior mitral line (AML). If required, additional epicardial ablation was undertaken to establish PVI, and block the LA inferior and roof lines and an AML.
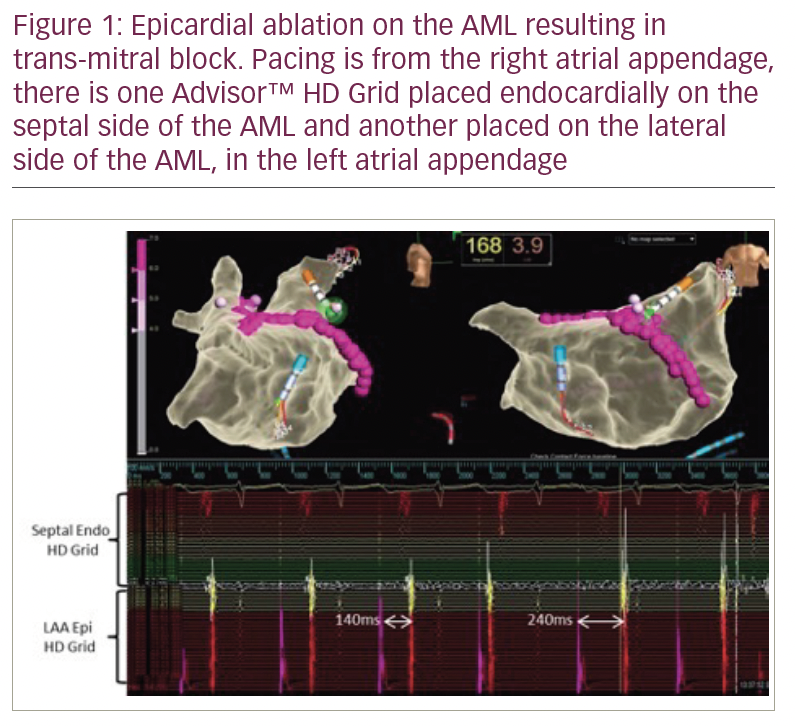
Results: Epicardial access was successful in all 11 patients, with less than 5 mls epicardial bleeding, as was epicardial mapping of the LA using both the transverse and oblique pericardial sinuses. Endocardial ablation alone achieved block in 73% (8 of 11) of roof lines, 91% (10 of 11) of inferior lines and 18% (2 of 11) of AMLs. Epicardial ablation directed on the roof line was required to achieve block in 1 case, and on the upper third of the AML to achieve roof line block in 2 cases. Epicardial ablation of the inferior line was required in 1 case to achieve block. In 9 cases, epicardial ablation directly on the AML was required to achieve trans-mitral block (Figure 1). Of the 9 reconnected pulmonary veins following prior PVI, 8 of 9 were reisolated with endocardial ablation and 1, a left upper PV, required epicardial ablation to achieve isolation.
Discussion: Use of the percutaneous subxiphoid pericardial CO2 insufflation technique to achieve epicardial access for LA mapping and ablation is feasible, and safe whilst on uninterrupted anticoagulation. Limited success in ablation for PsAF beyond PVI may be due to difficulty in creating trans-mural linear lesions. Epicardial ablation can be safely performed to achieve linear block in the roof, anterior and inferior LA. Epicardial structures such as the septopulmonary bundle may contribute to difficulty blocking roof lines endocardially, and account for remote isolation of the roof line via epicardial ablation on the AML.