Background: Determining the mechanisms driving atrial fibrillation (AF) during clinical procedures remains challenging. RETRO-map enables the analysis of intracardiac electrograms (EGM) to display activation maps during AF. We used RETRO-map to study the impact of circumferential pulmonary vein ablation (CPVA) on activation patterns in persistent AF.
Methods: Patients undergoing CPVA for persistent AF using the Precision™ 3D navigation system were recruited. An AFocusII catheter was positioned on the left atrial endocardium and 30 s of AF was recorded at multiple sites prior to CPVA. Following CPVA, this was repeated at the same locations. The data were exported to a custom-written MatLab program and analysed. The RETRO-mapping algorithm produced continuous activation maps and screened 2 ms time windows for evidence of focal activation, planar waves and wavefront collisions. These automated categorisations were manually validated and compared between pre/post CPVA using a standard T-test.
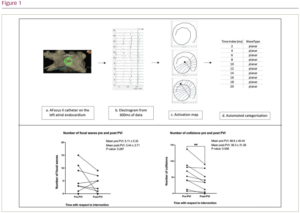
Results: Ten patients with a mean age of 61.3 ± 12.1 years (80% male) were recruited. The mean duration of persistent AF was 23 (9–51) months and the mean left atrial diameter was 45.0 ± 4.7 mm. Overall, 115 data segments were recorded from 61 different locations in these 10 patients. Using 3 s of data from each segment, 53 focal waves, 652 planar waves and 168 collisions were identified and manually validated. RETRO-map was highly effective at identifying focal waves and collisions, achieving 100% correlation with manual validation within the 2 ms time windows. For planar waves, the RETRO-map planar categorisation had to occur in 12 consecutive time windows (≥24 ms duration) to achieve an 80.3% correlation with manual validation. Comparing pre- and post-PVI recordings, the mean number of collisions significantly reduced (21.3 × 10-6 collisions/mm2/s/patient pre-PVI to 13.9 × 10-6 collisions/mm2/s/patient post-PVI; p=0.006). PVI decreased the number of focal activations (1.86 × 10-6 focals/mm2/s/patient pre-PVI to 1.17 × 10-6 focals/mm2/s/patient post-PVI; p=0.287), and it had no effect on the manually validated planar waves (16.0 × 10-6 planars/mm2/s/patient pre-PVI vs 16.1 × 10-6 planars/mm2/s/patient post-PVI).
Conclusion: RETRO-mapping showed that circumferential pulmonary vein ablation caused a reduction in wavefront collision. With larger series and additional ablation sets, RETRO-mapping may be able to determine the mechanisms maintaining AF.