Background: Elderly patients with atrial fibrillation (AF) may present with acute thromboembolic events, often in combination with high bleeding risk. There are limited data on such high-risk patients from China, as well as the benefits and harms of oral anticoagulants (OAC).
Objective: To investigate the impacts on death, thromboembolism (TE), and acute coronary artery syndrome (ACS) of different antithrombotic treatment strategies in elderly patients with AF with recent acute thromboembolism and at high risk for bleeding.
Methods: Chinese Optimal Thrombophylaxis in the Elderly patients with Atrial Fibrillation (ChiOTEAF Registry) was a prospectively, real-world registry from 44 research centres across China between Oct 2014 to Dec 2018. A Cox proportional hazard model analysis was performed for the outcomes related to antithrombotic therapy.
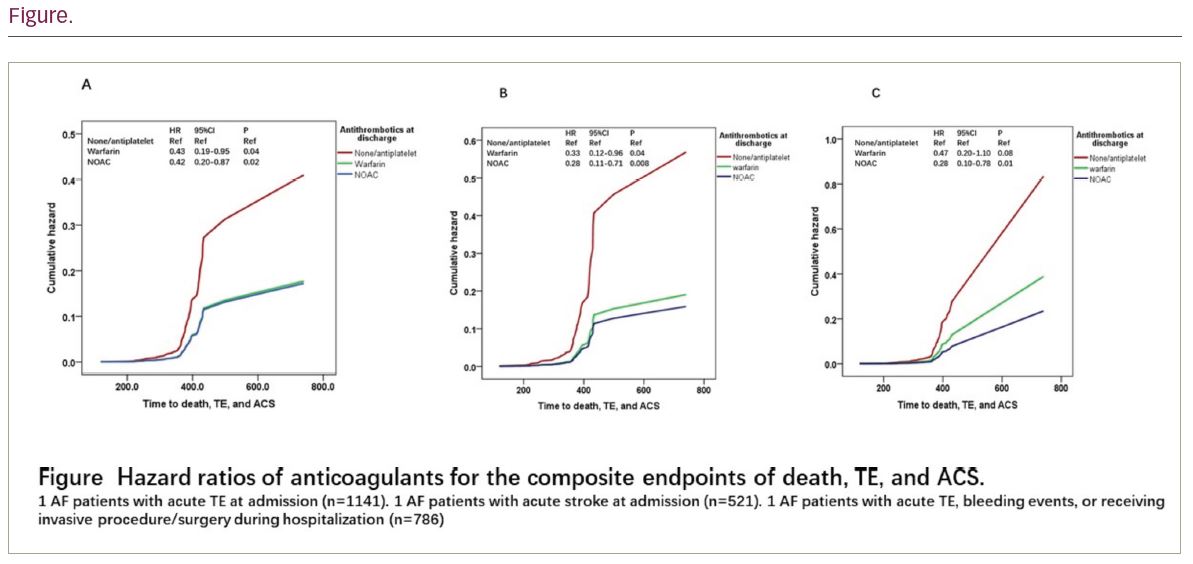
Results: There were 1141 patients (mean age 77 (SD 9) years; 42.3% female) presenting with acute thromboembolism (521 ischaemic stroke, 86 systemic thromboembolism, 664 ACS; of these, 1018 sustained single TE, 116 dual TE events, and 7 triple TE) at enrolment, with follow-up (mean ± SD) of 369 (54) days. CHA2DS2-VASc and HAS-BLED scores (mean ± SD) were 4.5 ± 1.6, and 2.8 ± 1.1 in this population, respectively. Among these, there were 786 (68.9%) AF patients with bleeding events or receiving invasive procedure/ surgery during hospitalization. During one-year follow-up, there were 57 (5.0%) deaths, 31 (2.7%) thromboembolism, and 14 (1.2%) ACS, while there were 4 (0.4%) intracranial haemorrhage and 15 (1.3%) extracranial haemorrhage. The usage (n, %) of oral anticoagulants (OACs), parenteral anticoagulant, and antiplatelet at discharge were 434 (38.0%), 80 (7.0%), and 707 (62.0%), respectively. After adjusting for age, gender, heart failure, hypertension, diabetes mellitus, prior myocardial infarction, chronic renal dysfunction, liver dysfunction, OACs at discharge reduced the risk for all-cause death, thromboembolism, and ACS (hazard ratio, HR, 95% confidence interval, CI) for the whole cohort (HR, 95% CI, 0.43, 0.19-0.95, p=0.04 on warfarin; 0.42, 0.20-0.87, p=0.02 on non-vitamin K antagonist OACs, NOAC, respectively). Subgroup analyses showed that the decreased risks for all-cause death, thromboembolism, and ACS of OACs were in AF patients with acute ischaemic stroke (all p<0.05), but not in AF patients with ACS. For AF patients with bleeding events, or receiving invasive procedure/surgery during hospitalization, NOAC at discharge decreased the risk for all-cause death, thromboembolism, and ACS (HR, 95% CI, 0.28, 0.10-0.78, p= 0.01).
Conclusion: Elderly atrial fibrillation patients with recent thromboembolism and at high bleeding risk derive benefits from OACs at discharge, especially amongst those with recent ischaemic stroke and with NOAC use.