Introduction: Surgical “Maze” was first performed in 1987, although techniques have evolved since then. The most recent 2017 Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation (AF) recommends concomitant ablation for symptomatic AF alongside other cardiac surgery (Class I/IIa) and standalone ablation (Class IIa) for persistent and long-standing persistent AF. We sought to evaluate the contemporary performance of surgical ablation at our centre.
Methods: Retrospective electronic database and case note review at a single tertiary centre, including all operations involving surgical AF ablation between January 2016 to December 2018. A 90 day “blanking period” was allowed post op. Of 278 patients initially identified, 94 were excluded as there was no follow up after initial clinic visit 90 days post-surgery. Follow up was for minimum 6 months, median 12 months. Cardiac rhythm was determined on 12 lead ECG pre-op and during post op follow up by Holter monitor and/or 12 lead ECG.
Results: Of 184 patients studied 115 were male (63%), with a mean age of 71 ± 11 years. 144 (78%) had persistent AF. 82 patients had hypertension, 21 had diabetes, 14 had chronic pulmonary disease, 19 patients had a previous myocardial infarction. 161 had a left ventricular ejection fraction (LVEF) of > 50%, 21 had LVEF 30-50% and 2 had LVEF < 30%. Mean left atrial size was 57 ± 15mm. 66 patients had mitral valve disease, 29 had aortic valve disease, 41 had disease of > 2 valves. Ablation performed ranged from pulmonary vein isolation only to Cox Maze IV. 33 patients had standalone AF surgery; in 116 ablation was combined with valve surgery, in 15 with CABG, in 20 with CABG and valve surgery. The left atrial appendage was treated by excision or clip device in the majority.
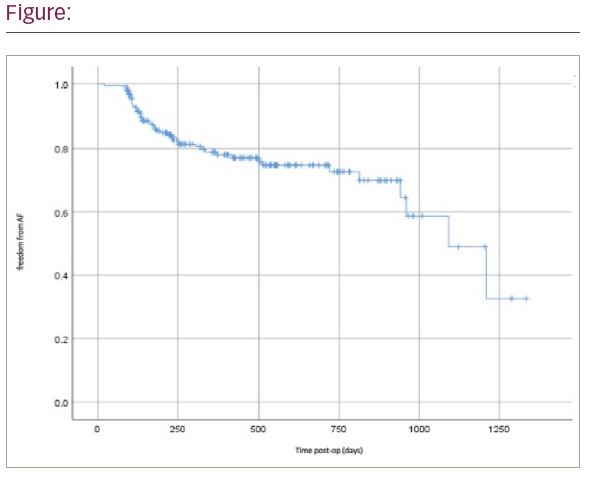
140 (76.1%) patients remained free of AF at last follow up. Figure 1 shows Kaplan-Meier curve for AF recurrence. Recurrence of AF in 44 patients occurred at a median of 212 days post op (range 91-1092). 7 patients underwent further catheter-based ablation. 30-day mortality was 3.6% and overall survival was 96%.
Conclusions: These data confirm excellent “real world” outcomes from surgical ablation in a cohort of mainly persistent AF patients, despite advanced atrial myopathy based on left atrial size, coexistent valve disease and comorbidity. The limitations are in its retrospective nature, involving a heterogeneous population and surgical lesion sets, with inconsistent use of Holter monitoring during follow up.