Introduction: Strategic implantable cardioverter defibrillator (ICD) programming, with the use of high-rate detection zones and long detection times, can significantly reduce non-essential ICD therapy and mortality. Despite the published data and guideline recommendations, the implementation of strategic programming into clinical practice has been modest. Here we describe our approach to improve ICD programming and its impact on the uptake of evidence-based programming in our institution.
Method: We introduced 3 specific strategies to improve adherence to evidence-based programming: 1. In late 2013 we introduced institutional ICD programming guidelines based on published data. Guidelines were circulated and compliance encouraged. 2. At the start of 2017 printed summaries of the guidelines were attached to all device programmers in the hospital and displayed on the wall in device clinic. 3. At the start of 2018 a monthly feedback and audit report on guideline compliance was circulated via email within the department. Results from the audit were graphically displayed in the device clinic on a bi-annual basis. In this analysis we included consecutive patients who received a new (or upgrade) ICD for any indication (January 2009 – December 2019) at King’s College Hospital (KCH), London. We evaluated implant programming with respect to KCH guideline compliance and the use of 2 specific evidence-based standards:
- High detection zones (defined as ≥180 bpm) in primary prevention patients
- Long detection times
We divided patients into 3 groups based on time:
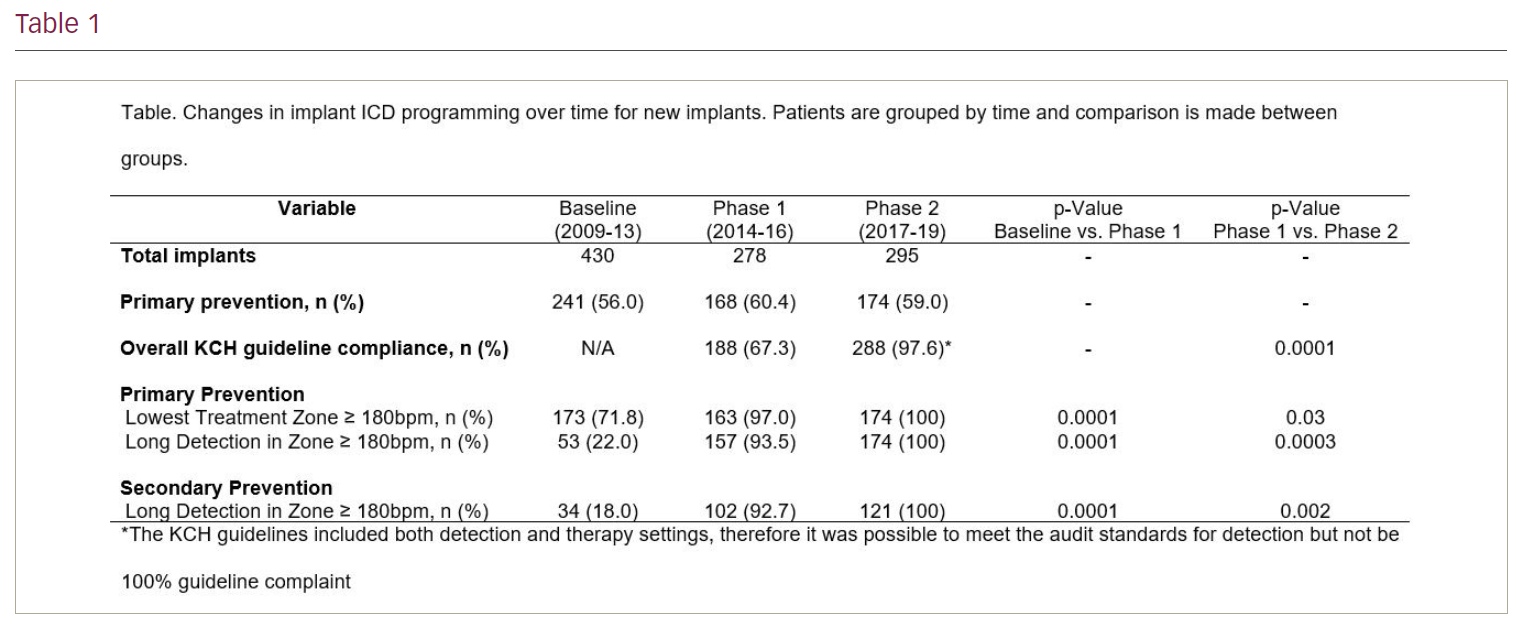
- Baseline – implanted 2009–13 prior to introduction of programming guidelines
- Phase 1 – implanted 2014–16 after KCH programming guideline introduction
- Phase 2 – implanted 2017–19 after KCH guidelines attached to programmers and feedback audit introduced.
Programming was compared between the 3 groups using the chi-squared test.
Results: Compared with baseline, introduction of programming guidelines (Phase 1) was associated with a significant increase in the use of high detection zones (97.0% vs 71.8%; p=0.0001) and long detection times (93.5% vs 22%; p=0.0001) in primary prevention patients, and long detection times (92.7% vs 18.0%; p=0.0001) in secondary prevention patients (Table). Following introduction of the printed programming guidelines and the monthly audit (Phase 2), compared with Phase 1 there was a further incremental increase in the use of high detection zones (100% vs 97.0%; p=0.03) and long detection times (100% vs 93.5%; p=0.0003) in primary prevention patients, and long detection times (100% vs 92.7%; p=0.002) in secondary prevention patients.
Discussion: The main finding of this study was that the use of a series of simple strategies was associated with a significant increase in the use of evidence-based ICD programming. Introduction of a departmental programming guideline increased the use of high detection zones and long detection times above 90% for new implants, with a further increase to 100% by increasing visibility of the guideline and providing a regular audit of performance. Our study demonstrates that relatively simple measures can make large differences to ICD programming. Furthermore, it is possible that the development of local guidelines achieved greater ‘buy-in’ from implanters than using international guidelines alone and contributed to the high levels of evidence-based programming achieved in our centre. ❑