Introduction: In the past decades, a significant association between the autonomic nervous system and cardiovascular mortality, including sudden cardiac death, has been recognised. Experimental evidence of an association between the propensity for fatal arrhythmias and signs of increased sympathetic or decreased vagal activity has encouraged the development of quantitative markers of autonomic activity. Heart rate variability (HRV) is well established and has been shown to be deteriorated in individuals with known structural heart disease. The present work is a first to compare HRV in ischaemic (ICM) and dilated (DCM) cardiomyopathy with focus on circadian and gender differences using both classical time-domain parameters and non-linear time domain as well as non-linear methods of fractal geometry.
Methods: A database of 923 Holter electrocardiograms (ECGs) from patients with ICM or DCM was reviewed to create comparable groups in terms of New York Heart Association class III–IV, left ventricular ejection fraction (LVEF) less than 40%, medication, gender and age. In order to analyse the circadian differences between patients with DCM and ICM, a 1-hour interval was selected during the day and at night for every patient (day from 6 am to 9 pm; night 9 pm to 6 am). Time intervals for final analysis were selected after visual confirmation. Artefacts were identified as such after visual discrimination. Measurements were conducted by linear and non-linear parameters during sinus rhythm.
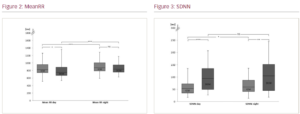
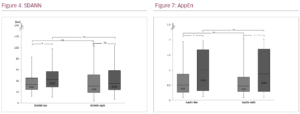
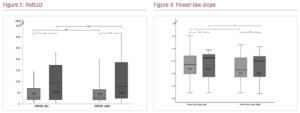
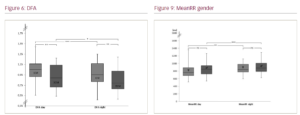
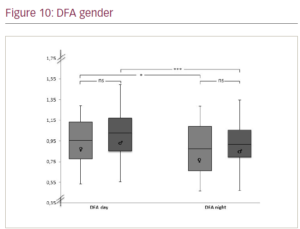
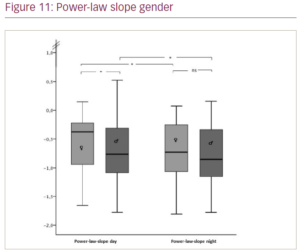
Results: Holter ECG recordings of 113 patients with structural heart disease (DCM n=38, mean age 67 ± 14 years; ICM n=75, mean age 72 ± 11 years) entered final analysis. Groups were comparable in baseline characteristics. Overall, 77 were male. Participants were on optimal medical treatment including medication with known antiarrhythmic effect in structural heart disease (ACE, ARB, beta blockers, no other class antiarrhythmic drugs), diuretics and MCRA; patients with ICM had additional dual antiplatelet inhibition and statins or ASA/statin therapy, with additional inconsistent ASA/statin administration in DCM patients. Figures 1–11 show the results with significances for our observations as follows: * (p<0.05), ** (p<0.010), *** (p<0.001) and n.s. (not significant, p>0.050).
Conclusions: Although the patients with DCM are clinically comparable in terms of cardiac function (mean LVEF of both groups 28%), medication and age, they appear to have higher heart rate variability compared with patients with ICM. Comparing gender differences, only a significantly steeper power law slope for men with structural heart disease was evident during the day. Whereas the observations regarding patients with DCM may come as a surprise, with only a slightly younger age as possible explanation, the observation for gender differences may be expected. ❑