Introduction: Pacemaker implantation and atrioventricular node (AVN) ablation is the last option for rate control of atrial fibrillation (AF) in patients unresponsive or intolerant to intensive rate and rhythm control and not eligible for rhythm control by pulmonary vein isolation (Class IIa indication in the European Society of Cardiology guidelines). Conduction system pacing is slowly evolving as an alternative to cardiac resynchronization therapy (CRT) pacing in these patients, providing a better physiological pacing and better haemodynamic response.
We present the case of a 69-year-old female patient with a history of persistent AF. She underwent two ablations, which were not sufficient to control her AF. In addition, she underwent four direct current cardioversions (DCCVs) in the last year. Rhythm control was not achieved with medications and the patient suffered from severe intolerance to beta-blockers and sotalol. As the patient’s desire was to end these ‘regular’ visits to A&E for DCCVs and to stop medical treatment too, we offered to proceed with native conduction system pacing and AVN ablation.
Methods: The following stepwise approach was taken.
I. Pacing
1. Narrow complex in sinus rhythm. Measurements of HV, QRS and H-end QRS intervals.
2. Looking for selective His pacing (distal His) leading to equivalent P-V, QRS and P-end QRS intervals.
3. Screwing in of the His pacing lead at the abovementioned position. If pacemaker parameters are good and there is no change in the His capture, proceed to AV node ablation.
4. If the threshold at this position is high or if there is no good native conduction system capture with narrow QRS at distal His, proceed to LBBA pacing.
5. Move the lead approximately 1 cm lower on the septum in apical direction.
6. Starting septal RV pacing with ‘W shape QRS’ in V1.
7. Start screwing the lead with special focus on PVCs and impedance.
a) Once we see any RBB looking PVC, we stop.
b) Also after 10 turns, we stop and pace.
c) Continue until we see a tall R in V1 – this means we captured the LBB.
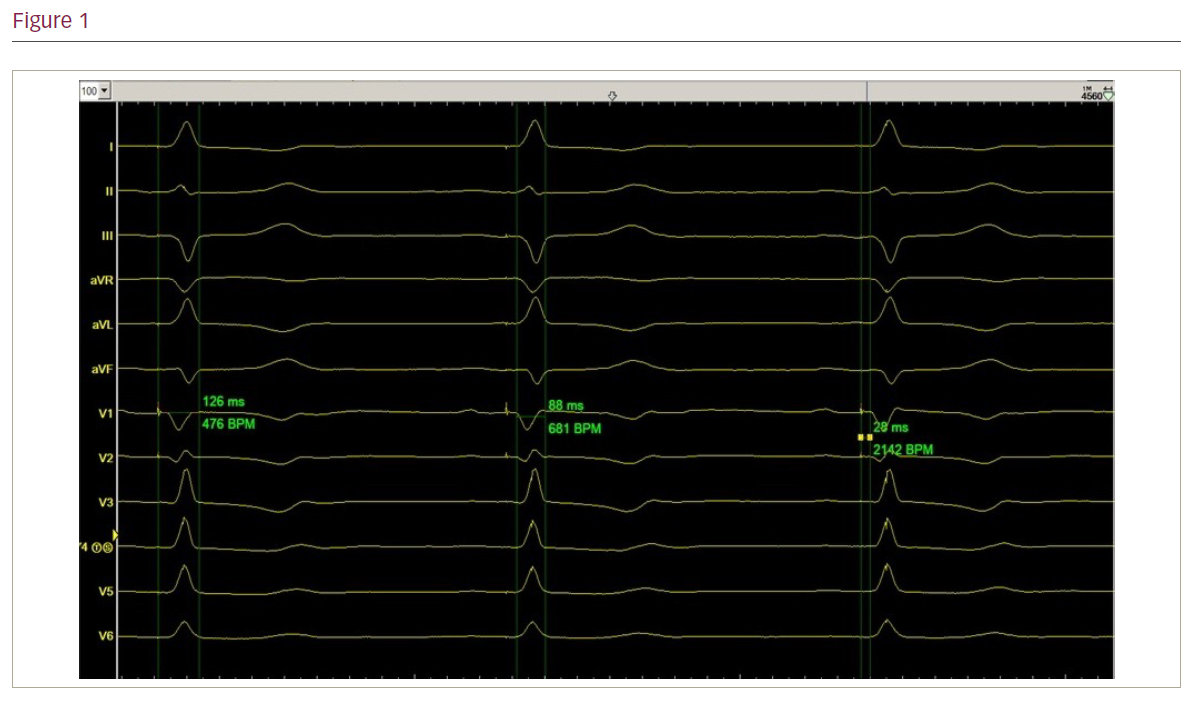
8. Aim for LBB potential on intracardiac EGM – sharp positive deflection before the QRS – ‘bull’s eye’.
9. Important measurements during LBB mapping and pacing:
a) PS to QRS <40 ms
b) PS to peak QRS in V5 <80 ms
c) PS to end QRS <130 ms.
10. Contrast injection to assess the depth of the lead into the septum.
11. If pacemaker parameters are good and there is no change in the LBB capture, proceed to AV node ablation.
II. Ablation
1. Do not dislocate the pacemaker leads!
2. LV pacing at VVI 40 bpm.
3. Target the proximal His bundle – proximal ablation side allows narrow complex escape rhythm too and is far from His/LBBA pacing lead.
4. Ablate for 30 seconds while achieving CHB in the process.
Results and conclusion: In this patient, we achieved a LBBAP with final ECG intervals similar to the baseline ECG before the procedure. This allowed better physiological pacing compared with dual-chamber pacing and CRT with a better haemodynamic response. ❑