Introduction: Guidelines recommend the implantation of primary prevention defibrillators (pICD) in patients with a left ventricular ejection fraction (LVEF) of <35% due to the associated higher risk of ventricular arrhythmias (VA) in this cohort. However, reported incidence of VA in this cohort is only 5–10%/year with many deaths occurring prior to VA events and up to 2/3 of patients receiving no appropriate intervention over the lifetime of the device. Post hoc analysis of 4 prospective MADIT trials (4,531 patients, 2002–2012) developed a predictive model containing 12 unique variables to assist in patient stratification according to benefit obtained from pICD over a 3-year period. Outcomes predicted included identifying those at the greatest risk of VA or non-arrhythmic mortality without prior arrhythmia (NAM). This was validated on data from the RAID trial (2011-15). We assessed the performance of the MADIT ICD Benefit score on a ‘real-world’ cohort and correlation of the predictive value of each variable.
Methods: We undertook an observational study applying the MADIT ICD Benefit score to consecutive new pICD and cardiac resynchronization therapy defibrillator (CRT-D) implants of ischaemic and non-ischaemic aetiology and LVEF <35% between 2014 and 2019 at a single UK tertiary centre. The primary outcome was first VA or all-cause mortality without prior ventricular arrhythmia (NAM). VA was defined as any treated VA, any sustained VA that was monitored only or ventricular fibrillation. Follow-up data were gathered for a maximum 3-year follow-up period. Kaplan–Meier survival curves separated by MADIT Benefit group were compared for each event. Assessment of each score variable was undertaken with Cox proportional analysis.
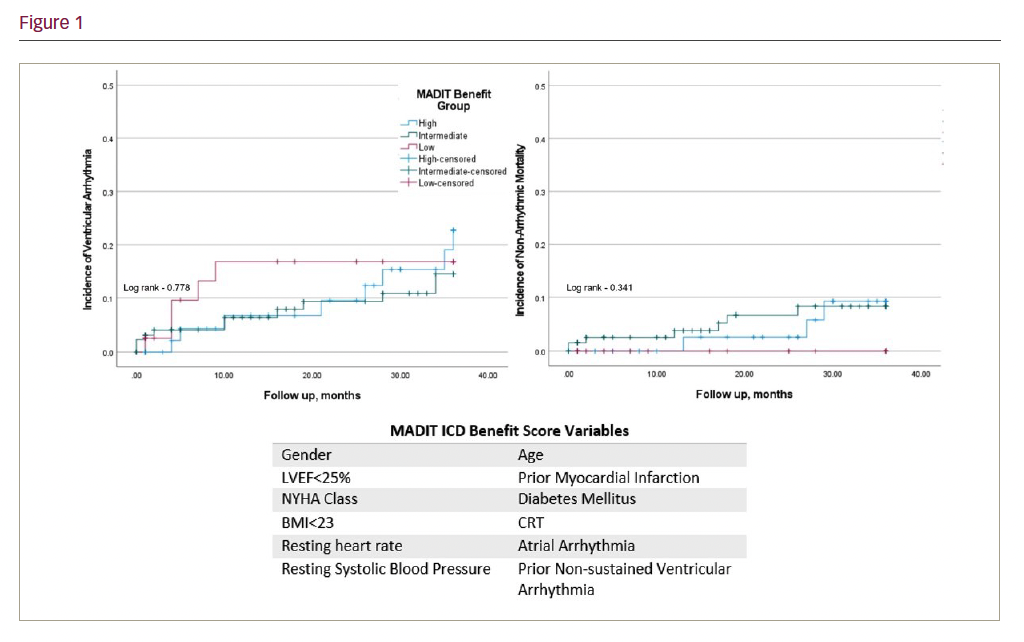
Results: Out of 576 primary prevention implants, 228 had the requisite complete data for score calculation. Mean age was 66.3 ± 12.3 years, 78.1% were male, 61% received a CRT-D and 44.7% had an LVEF <25%. Aetiologies were ischaemic (52%) and dilated (48%) cardiomyopathy. There were 25 VA events and 10 NAM occurred over a median 25 months’ follow-up. At 3 years, there was no significant difference between high, intermediate or low benefit groups for incidence of VA (22.7%, 14.5% and 16.8%, respectively; p=0.778) or NAM (9.2%, 8.3% and 0%, respectively; p=0.341). Statistically significant predictive factors for VA were gender (HR 4.24, CI 1.01–17.76; p<0.05) and previous non-sustained VA (HR 4.18, CI 1.92–9.1; p<0.01). None of the model variables were linked with predictive factors of non-arrhythmic mortality.
Conclusion: The MADIT ICD Benefit score was unable to accurately stratify patients according to arrhythmic or mortality risk. Furthermore, only 4 variables were associated with VA and none with NAM. Our dataset had significant variation to the original training set including a higher proportion of non-ischaemic cardiomyopathy (48% vs 34%, respectively), higher CRT implants (61% vs 40%) and higher rates of atrial arrhythmia (30.3% vs 14%). Despite this, our data are representative of guideline adhered practice. The MADIT ICD Benefit Score was not applicable to our local data. This may be representative of the impact of advancing heart failure management and services on patients, a population change resulting in non-generalisability of a scoring system based on older studies. Additional heart failure medication data are being collected locally for assessment, but larger, multicentre studies would be required to confirm this hypothesis.