Introduction: Atrial fibrillation and heart failure often coexist, and are associated with increased morbidity and mortality. Their temporal association may not always be clear, with clinicians often facing a ‘chicken-or-egg dilemma’. In this cohort of patients with persistent AF and LV dysfunction, electrical cardioversion is often undertaken to elucidate the aetiology of the LV dysfunction and guide further therapy. Recurrences of AF post cardioversion are common and can be reduced with anti-arrhythmic drugs. NICE guidelines suggest that pre-treatment with amiodarone is considered prior to cardioversion, but do not specify clinical indications where its use would be required as first-line. This could explain a degree of variation in the use of amiodarone pre-treatment in this group noted in the local cardioversion service that led to this retrospective study.
Methods: Retrospective data was collected for patients referred for electrical cardioversion between January 2020 and August 2022 with persistent AF or flutter and LV ejection fraction ≤45%. We compared the success rate of external DCCV in achieving sinus rhythm acutely and its maintenance at follow-up (8 ± 5 weeks) between the cohorts of patients undergoing cardioversion without amiodarone pre-treatment and patients undergoing cardioversion with amiodarone pre-treatment (including patients that chemically cardioverted following amiodarone initiation and that had a first cardioversion without amiodarone).
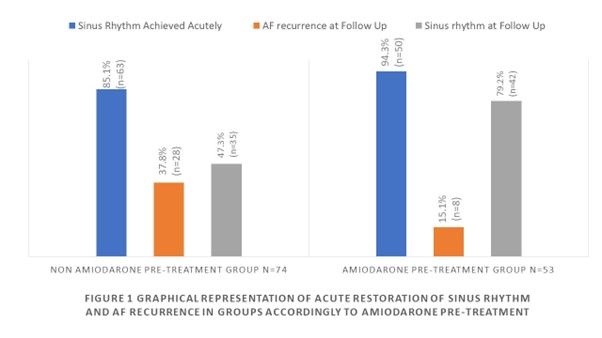
Results: Ninety-nine patients fitted the inclusion criteria. Of these, 79 patients were male and 20 were female. The mean age was 68.2 ± 9.8 years. The mean LV EF at time of referral was 31.7 ± 7.8%. The acute success of cardioversion and rhythm at follow-up are outlined in Figure 1. In the cohort pre-treated with amiodarone, 7/53 (13.2%) patients achieved chemical cardioversion prior to their external DCCV. Twenty-eight patients (37.8%) not initially pre-treaded with amiodarone had a second cardioversion on amiodarone. Twenty-eight out of 74 patients (37.8%) and 8/53 patients (15.1%) in the non-amiodarone pre-treated group and amiodarone pretreated group respectively relapsed back into AF. There was a statistically significant lower rate of recurrence in patients treated with amiodarone (15.1% versus 37.8%, p-value <0.05). The relative risk of AF recurrence was 0.36 (95% confidence level, p value 0.001917) when amiodarone was used.
Discussion: This study demonstrated that patients with LV dysfunction are at high risk of early AF recurrence and often require an early repeat cardioversion on amiodarone. A lower relative risk of AF recurrence was observed at the initial follow-up among patients who had cardioversion on amiodarone. First-line amiodarone pre-treatment can lead to earlier maintenance of sinus rhythm, thus abetting earlier diagnosis of LV dysfunction aetiology and support decisions on further treatment. This practice can avoid the need for repeated DCCVs, resulting in more efficient use of NHS resources. In this group, clinical trials such as CASTLE-AF and EAST-AFNET4 demonstrated that rhythm control with catheter ablation leads to improved outcomes. In the current context of long waiting times for catheter ablation, this can be an effective bridging treatment.
Limitations: This was a non-blinded, non-randomized, retrospective, observational study that did not evaluate adverse effects or considered other risk factors for AF recurrence. Thus, further studies into the safety and outcomes of initial amiodarone treatment are needed. ❑
Figure 1: Graphical representation of acute restoration of sinus rhythm and AF recurrence in groups according to amiodarone pre-treatment