Introduction: The Cardiac Physiology led implantable Loop recorder (ILR) service has seen a yearly increase of implants over the past 3 years from 48 to 224. We therefore predict that due to the 3-year battery life of the device, explant referrals will increase. This traditionally has been physician led in the cath lab utilising a day case bed. Here in we present a Physiologist-led ILR explant service in a non-cath lab environment.
Aim: To examine prospectively the Cardiac Physiologist (CP) led ILR explant service.
Method: The lead CP was trained over 2 months and a second implanter trained. A review of 20 patients was set in order to determine the suitability of moving the explant procedure out of the Cath Lab where X-Rays will not be available. Ten patients had their procedure performed in the cath lab and 10 in a procedure room.
Inclusion criteria for explants by physiologists included:
- age ≥ 16 years;
- Medtronic Reveal Linq in situ; and
- no specialised consultation required.
Anticoagulation was omitted 24 hours prior to the procedure, those patients who are unable to stop the anticoagulation were deemed unsuitable for this service. As per our implant policy, wounds are closed with one dissolvable suture, steri-strips and a dressing. No antibiotics are administered.
Results: Twenty ILRs were successfully explanted during November 2018 to April 2019. One patient required an X-Ray to confirm the location of the device, the X-Ray showed off label positioning. Of those explants performed in the cath lab, none required X-Ray to determine the device location.
Out of the 20 explants, there were no complications. No infections have been reported one-month post explant.
Performing explants in a procedure room, saved 2 days cath lab for other invasive procedures, and a cost saving of £1030 per patient, see Figure 1.
Future: To allow the service to be “fit for the future” it is predicted that the service needs two trained CP to explant a minimum of six devices per month. This will not only reduce the patient waiting list, but it will also allow staff to maintain competence and confidence. We expect referral rates to increase, therefore regular reviews will be taken place and further CPs trained to perform ILR explant in order to ensure the service doesn’t become suitable for capacity.
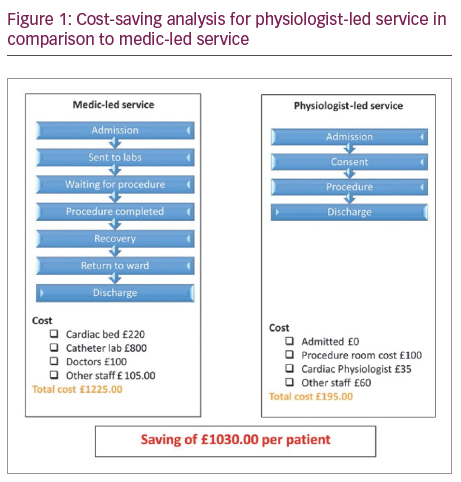
Taking into consideration the 2018 explant procedures (n=70) we expect to save the Trust a minimum of £73,130 per year. We predict a significant increase in explant referrals as the service develops which will see cost saving to further improve.
Conclusion: A physiologist-led ILR explant service in a non-catheter lab setting is a safe alternative to a medic led service with significant cost saving for the Trust.