




Highlights
-
Failure to target and deliver durable radiofrequency lesions to all functionally critical areas has been identified as an important cause of ventricular tachycardia recurrence and is particularly challenging in deep midmyocardial or very extensive substrate where point-by-point radiofrequency ablation becomes impractical.
-
Alternative approaches have been described to: improve radiofrequency energy delivery to the tissue to achieve deeper and more durable lesions; use alternative energy sources and delivery modes for physical as well as chemical ablation; and address proarrhythmogenic aspects of the autonomous nervous system.
-
Improved mechanistic understanding of ventricular arrhythmias and detailed preprocedural structural and electrophysiological substrate characterization will allow identification of patients with difficult and complex substrates beforehand and may inform tailored procedural approaches to improve success rate and arrhythmia-free survival.
-
With growing experience and widespread use of ventricular tachycardia ablation, the complexity of substrates and patient profiles being offered a ventricular tachycardia ablation also increases. Depending on local experience, options for additional and/or complementary interventional treatments should be considered upfront at the index procedure
Percutaneous catheter ablation has an established role in the management of ventricular arrhythmias (VAs) to prevent recurrence and implantable cardioverter/defibrillator shocks. Yet, despite the progress in our mechanistic understanding and visualization of the arrhythmogenic substrate to inform ablation strategies as well as technological advances in electro-anatomical mapping and ablation technology, procedural success rates remain moderate. The lack of unequivocal prognostic benefit and substantial ventricular tachycardia (VT) recurrence in the long-term follow up raises the question whether the traditionally used point-by-point radiofrequency ablation (RFA) might not be the appropriate tool to eliminate the arrhythmogenic substrate in all patients. Several new ablation technologies have been proposed to overcome existing limitations and offer possibilities of a more tailored approach guided by the specific characteristics of each patient’s unique arrhythmogenic substrate.
Preprocedural preparation and existing radiofrequency technology
Individualized ablation approaches require thorough pre- and intraprocedural substrate characterization to inform selection of the most suitable ablation modality and delivery mode. Options for state-of-the-art assessment of the underlying structural and electrophysiological alterations in patients with VT are summarized in Figure 1. This is of particular importance in the complex and heterogenous group of nonischaemic cardiomyopathies. The latter have been found to have consistently higher procedure failure and VT recurrence rates after catheter ablation than patients with ischaemic heart disease, not least due their frequently mid- and subepicardial substrate likely requiring different ablation approaches than standard RF ablation.1
Figure 1: Overview of arrhythmogenic substrate characterization
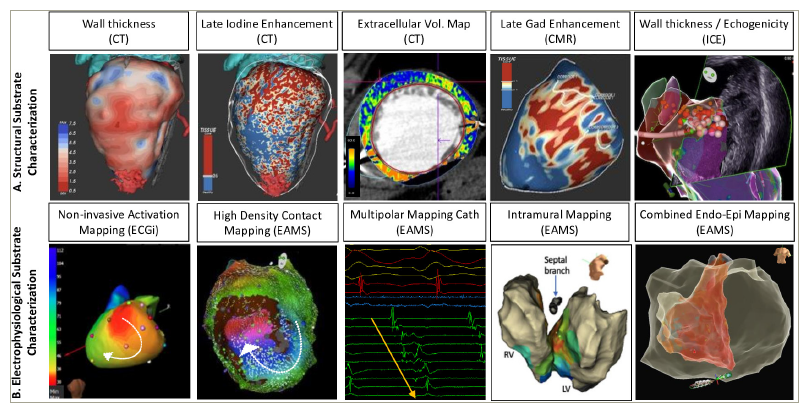
A. Structural: Multiple imaging modalities are available to characterize the underlying structural substrate of ventricular arrhythmias including (from left to right) preprocedural computerized tomography scans of wall thickness, late iodine enhancement, extracellular volume maps (orange = high ECV representing scar), cardiovascular magnetic resonance late gadolinium enhancement models (red = representing scar) and intraprocedural intracardiac echocardiography. B. Electrophysiological: Characterization of the functional electrical ventricular tachycardia substrate can be achieved by (from left to right) noninvasive activation mapping with electrocardiographic imaging (CardioInsightTM, Medtronic, Minneapolis, US), invasive high-density contact mapping using dedicated multipolar mapping catheter and novel algorithms to delineate areas of late activation and deceleration, as well as employing intramural and combined endo-epicardial mapping approaches.
CT = computerized tomography; CMR = cardiac magnetic resonance; EAMS = electro-anatomical mapping systems; ECGi = electrocardiographic imaging; ICE = intracardiac echocardiography.
Options for existing and advanced RF delivery strategies to target challenging VT substrates are summarized in Figure 2.2–5 They involve impedance modulation using hypotonic6 or nonionic irrigation,7 modification of location and number of dispersive patches,8 high-power long-duration lesions,9 and combinations of simultaneous unipolar ablations10 or true bipolar ablation.11 Investigational devices for intramyocardial RF delivery over extendable RF needles12 and wires5 or larger continuous ventricular lesions via linear2 or spherical13 ablation catheter designs have also been proposed. These approaches have been reviewed.14–16
Figure 2: Investigational radiofrequency ablation devices and delivery modes to maximize lesion dimensions
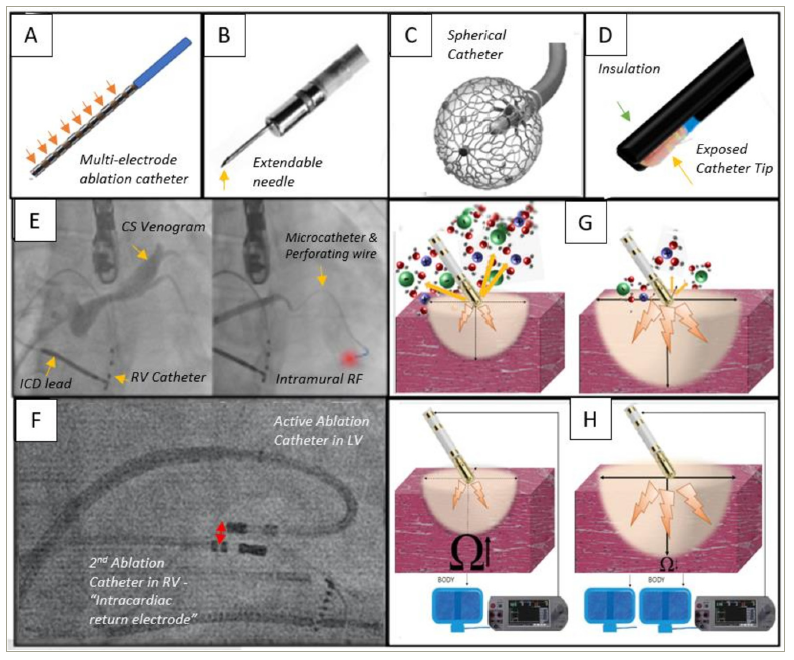
A.Schematic illustration of a linear radiofrequency ablation catheters (as originally proposed by Nazer et al.2) B. Extendable radiofrequency needle (adjusted from Stevenson et al.3, modified and reprinted with permission of the authors) C. Spherical radiofrequency catheter (reprinted with permission of Affera Inc., Medtronic, Newton, MA, USA, not approved for use in the ventricle). D.Schematic representation of a partially insulated radiofrequency catheter (as proposed by Nguyen et al.4) E. Coronary venogram with subsequent intentional coronary venous perforation for intramyocardial radiofrequency delivery over wire (as proposed by Romero et al.5). F. Fluoroscopy of true bipolar ablation on the intraventricular septum. G. Hypotonic irrigation to maximize radiofrequency dimension. H. Addition of a second dispersive patch to reduce system impedance to increase lesion size.
CS = coronary sinus; ICD = implantable cardioverter/defibrillator; LV = left ventricle; RF = radiofrequency; RV = right ventricle.
Alternative energy sources for ventricular tachycardia ablation
Ultra-low temperature cryoablation
Rational
Cryoablation in the ventricle is mostly known for its use in surgical ablation or the notoriously difficult to treat papillary muscle17 or moderator band VAs.18 Yet, lesion depth with focal cryoablation has remained an unresolved issue. A novel technology termed ultra-low temperature cryoablation (ULTC) has been proposed to overcome some of the major challenges of contemporary point-by-point ablation, including lesion depth and ablation duration. ULTC uses nitrogen that exist in the state between liquid and gaseous form as opposed to the traditionally used gaseous nitrous oxide. Theoretically this has been reported to generate temperatures as cold as -196°. The CE-marked system (Adagio Medical, Inc., CA, USA) include a console and dedicated 9Fr bidirectional VT ablation catheter with a 50 mm radius, a 15 mm cryoablation element and eight electrodes for intracardiac recordings (Figure 3). The catheter can be visualized in impedance-based localization systems. ULTC lesions can be applied over defined cryoablation cycles with fixed duration of first freeze (60–300 seconds), followed by a 60 second thaw and a second application at the same site.19
Figure 3: Ultra-low temperature cryoablation system
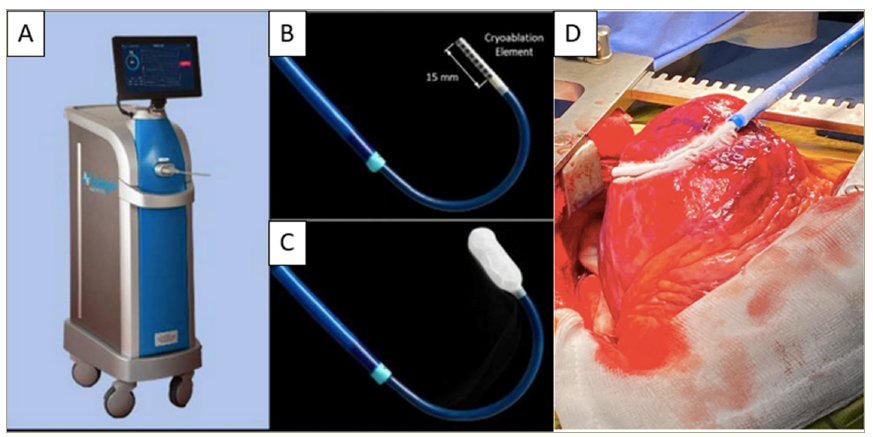
A. Cryoablation console. B. Ablation catheter with 15 mm cryoablation element. C. Ablation catheter with ice ball forming on cryoablation element. D. Traditional surgical cryoablation during open heart surgery via median sternotomy.
A–C reprinted with the permission of Adagio Medical Inc. CS-098, Laguna Hills, CA, USA. D. Image courtesy Dr John Silberbauer, Royal Sussex County Hospital, Brighton, UK.
Evidence
Initial preclinical studies (sheep/swine models) demonstrated that a single shot ULTC application creates contiguous myocardial lesions with a depth of 5.6 ± 2.2 mm without injury to surrounding tissues.20 With freeze-thaw-freeze cycles with total freeze time of up to 5 minutes, a lesion depth of up to 13.5 mm may be achievable as demonstrated by bench data testing conducted by the company. Yet transient coronary spasm was apparent when applied in the vicinity of coronary arteries.20–22 In the ventricle, a case series of the first patients of the ongoing first-in-human multicentre feasibility study (CryoCure-VT; ClinicalTrials.gov Identifier: NCT04893317) have been published with encouraging acute success rates.23–25 One pericardial effusion and an asymptomatic ventricular pseudoaneurysm were reported.
Ventricular tachycardia substrates to target with ultra-low temperature cryoablation
The wide region covered per freeze to interrupt critical parts of VT circuits from the endocardial surface alone make it a promising technique when extensive substrate modification is pursued and may shorten procedure time substantially. The cryo-adhesion effect together with deep lesion formation is also an ideal combination for targeting papillary muscle VTs (and indeed any site with difficult catheter stability and contact) originating from deep within the muscle.
Pulsed field ablation
Rational
The key advantage of this non-thermal energy causing electroporation is based on its tissue selectivity to promote targeted cell injury while minimizing risk of collateral damage to adjacent structures.
Evidence
Initial preclinical pulsed field ablation (PFA) studies were performed on the epicardium to investigate the relationship between energy delivery, lesion size and safety profile.26,27 Subsequent proof-of-concept investigations for endocardial ventricular PFA showed an average lesion depth of 6.5 mm with homogenous fibrosis and no interspersed viable myocardium, and no damage to nerve fascicle and vascular structures.28 Dose-finding studies in an animal infarct model using a bipolar biphasic PFA for 3 × 2.5 seconds over a linear quadripolar (‘focal’) and a multi-spline 8-pole basket catheter demonstrated significantly deeper lesions with PFA compared with RFA using either catheter (PFA 6.1 mm ± 1.7 mm compared with RFA 3.8 mm ± 1.7 mm).29 Repetitive applications of a similar electrical field were found to further increase lesion dimension to an average lesion depth of 8.8 mm.30 Importantly, PFA has been shown to also produce transmural lesions in the presence of heterogenous scar tissue with separating layers of collagen and fat; whereas, the insulating fat layers are a notoriously difficult challenge to overcome for RFA.31 Followed by these encouraging results, case reports for first-in-human PFA to treat scar-related VT have been published.32,33
Ventricular tachycardia substrate to target with pulsed field ablation
Tissue selectivity and the possibility of deep lesion creation have raised hopes to facilitate ablation of substrate located deep and/or insulated by intramural and epicardial fat and close to critical structures. Yet, reported coronary spasms during epicardial PFA have certainly raised concerns and highlighted that important questions for optimal dosage protocol and safety (as well as long-term efficacy) remain open.34 Most available PFA catheters (Figure 4) are approved for atrial but not yet for ventricular ablation.
Figure 4: Percutaneous and surgical pulsed field ablation catheters designs allow to adjust to anatomical and procedural requirements
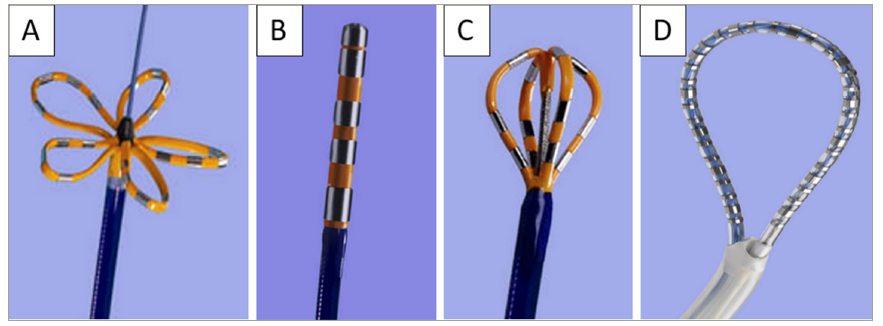
A. Flower shaped farawave catheter. B. Focal farapoint. C. Large area focal faraflex catheter. D. Surgical faraone catheter to create circumferential lesions around the pulmonary veins and posterior left atrium.
A–D reproduced with permission from Boston Scientific/Farapulse Inc., Menlo Park, CA, USA.
Combined pulsed field ablation and cryoablation
Despite being a non-thermal energy, at higher voltages transient heat generation in the vicinity of ablation electrodes and microbubble formation has been reported in PFA.35 ‘Precooling’ the tissue for 30 seconds followed by a concurrent biphasic bipolar PFA train has been suggested and tested in an animal study.36 A 8.5Fr non-deflectable ablation catheter with 20 electrodes, an insertable stylet to preshape according to the target zone, ULTC console and a PFA generator were used and achieved lesion depths of up to 6–7 mm. Opposed to PFA deliveries, which may cause muscle contractions and significant microbubble generation on intracardiac echocardiography, this did not occur with combined PFA and cryoablation.36
Photoablation
Rational
Laser ablation causes thermally induced coagulation following absorption of the laser light by the surrounding tissue without tissue vapourization. Recently, a custom-made irrigated 20 mm bidirectional 8.2Fr linear laser ablation catheter, with convex active laser area to prevent divergence and optimize wall contact (Vimecon GmbH, Herzogenrath, Germany), has been proposed for linear endocardial atrial (cavotricuspid isthmus) as well as epicardial ventricular ablations in an attempt to provide faster and deeper linear lesions sets than point-by-point RF.
Evidence
In animal studies using energy densities between 75 J/mm (cavotricuspid isthmus) and 150 J/mm (for ventricular myocardium), maximum lesion depth was reported to be up to 9 mm with a length of 25 ± 1.35 mm without any tissue oedema in the subsequent macroscopic analysis of the excised hearts (Figure 5).37 Furthermore, previous studies have shown that pulsed laser and a wavelength of 800 nm have a higher penetration (in comparison with 980 nm) and lesion depths could therefore be modulated as needed.38 No human data is available for laser ablation for VT ablations.
Figure 5:Illustration of laser ablation catheter and ablation lesions
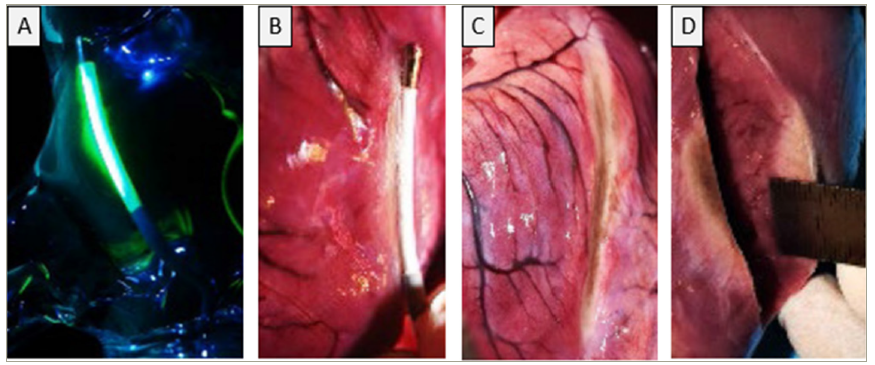
A. Custom-made linear laser active area visualized with low-energy green laser diode (Vimecon GmbH, Herzogenrath, Germany). B. Laser catheter positioned on the epicardium. C. Demonstrating the linear ablation lesion on the surface. D. Showing a lesion depth of 9 mm.
A–D reproduced from Krist et al.37 and reprinted under the CC BY licence.
Ventricular tachycardia substrate to target
The unidirectional emission of laser light can prevent collateral damage of adjacent structures and the existing optical fibre could allow the use of spectroscopy to directly visualize the tissue and lesion formation.37 Together with the possibility to titrate lesion depth via wavelength and the lack of tissue oedema, highly controlled lesion delivery to targets close to critical structures (such as the para-hissian area, coronaries and phrenic nerve) may become feasible. Furthermore, achieving transmurality at a given wall thickness in a safe and efficient way would be advantageous if subepicardial substrate is targeted from the endocardium alone (e.g. postcardiac surgery with inaccessible pericardial space). Lastly, durability of the lesion may be more predictable at the time of the procedure given the lack of oedema. The latter may occure with other energy sources and is often associated with reversible injury mimicking acute success but recovery of conduction over time.
Acoustic ablation: High-intensity focused ultrasound and shock wave catheter ablation
Rational
Interactions of the acoustical mechanical wave (compression and rarefaction that propagates within a medium) with tissue can be categorized into thermal (mediated by absorption and heat generation) and mechanical effects (due to acoustic pressure and force exerted on the tissue, movement of fluid in the pressure field [‘acoustic streaming’] and formation of gas filled cavities [‘cavitation’]).39 High-intensity focused ultrasound (HIFU) uses the thermal and shock wave ablation mechanical effect to target the underlying VT substrate.
High-intensity focused ultrasound evidence
In an open-chest animal study with the use of a custom-made HIFU probe, lesions of up to 15 mm in depth were achieved with ablation for 60 seconds, while coronary arteries were entirely spared even with applications directly on top of them.40 A follow-up study using subxiphoidal epicardial access reconfirmed that HIFU ablation over coronary arteries and surrounding epicardial fat is feasible and successfully achieves deep lesions while preserving normal angiographic flow.41 The latter may be explained by the substantially higher absorption of ultrasound energy in the myocardium than by blood. Feasibility of applying in vivo HIFU via an endocardial catheter based approach was demonstrated using a 3 × 5 mm transducer and successfully targeted deep septal substrate.42 Lesion volume decreased over the first 30 days yet transmurality increased by 58%, which was attributed to a reduction in septal thickness.
In a closed-chest animal model applying a noninvasive HIFU system, as it is clinically used to target human neoplasms43 , it was shown that with ablation energies of 400W for 2–4 seconds, transmural and localized lesions could be created without apparent injury to skin, lung or pericardium.44 Yet, thus far no human feasibility studies have been published.
Shock wave catheter ablation evidence
Low-energy extracorporeal shock wave therapy has been investigated as a noninvasive angiogenic, antianginal therapy for coronary artery disease.45 It was noted that focused shock waves could also cause tissue damage at an arbitrary depth without heat generation. As a consequence, high-energy shock waves to target the arrhythmogenic substrate of VT in the myocardium were suggested. The first in vivo animal studies of shock wave catheter ablation, which were applied over a custom-made prototype system by epicardial and endocardial approaches, demonstrated general feasibility; although, this was with only shallow lesions in the range of 2–3 mm and had concerns for microthrombus formation.46 A subsequent adjustment of the shock wave catheter ablation and alteration of irradiation numbers achieved had improved lesion depths of 6.5 ± 2.2 mm with 90 shots per site and without damage to the coronary arteries.47 At present, there is no human data available.
Ventricular tachycardia substrate to target with acoustic energy
Encouraging results of the surface and coronary sparing effect make acoustic ablation an interesting option for VT ablation at sites otherwise at prohibitive risk of iatrogenic coronary injury or covered by thick layers of epicardial fat (e.g. left ventricular summit). The noninvasive HIFU system may rival noninvasive radiotherapy in an attempt to minimize periprocedural morbidity and risk of complications of VT ablation while eliminating the arrhythmogenic source without the concerns of using ionizing radiation. Experience with HIFU in other medical disciplines (such as oncology), and existing commercialized HIFU systems may facilitate and inform translation into cardiological applications in the future. Yet the usual difficulties of applying precise noninvasive therapy to a moving target (cardiac/respiratory motion) apply.
Noninvasive ventricular tachycardia ablation: Stereotactic ablative radiotherapy
Rational
Stereotactic ablative radiotherapy (SABR or STAR, referred to as SABR in this article) is an established oncological treatment modality capable of delivering a compact, precise (in the submillimetre range) ablative radiation dose to the intended target in the body. Target zones are demarcated within a 3D coordinate system of a planning computerized tomography (CT) scan, with intentional steep gradients in all directions from the target to avoid damaging of adjacent tissue. This basic concept has been adapted to noninvasive treatment of VTs, aiming to deliver a potent ablative energy dose to functionally critical areas while minimizing procedural risk for the patient and collateral damage. The interaction of the ionizing radiation with the tissues results in DNA breaks and cell death, which ultimately induces electrically inert fibrosis.
Evidence
Various forms of ionizing radiation (such as photons, protons and carbon ions), dose protocols (5–160 Gy in single or multiple fractions) as well as target volumes have been explored for SABR. Clinically, photons are the most frequently used radiation. Based on initial preclinical dose-finding studies, standard target doses for SABR range around 25(–35) Gy delivered as a single fraction, which were shown to effectively create myocardial fibrosis while having an acceptable safety profile.48
After the first-in-human case reports49 and two landmark publications showing an impressive reduction in VT burden,50,51 SABR for VT ablation has rapidly gained widespread interest. Yet, subsequent retrospective52 and prospective studies,53–55 and the publication of long-term follow-up data cautioned a comparatively high rate of VT recurrence and high mortality due to heart failure, and rare but serious complications (such as late gastropericardial fistula, late pericardial effusions and pneumonitis).48 In clinical practice, a substantial variation in preprocedural workup in terms of imaging modality (cardiac magnetic resonance, nuclear imaging or CT), electrophysiological target definition (invasive electro-anatomical maps, electrocardiographic imaging or even just 12-lead electrocardiogram), and co-registration of the structural and electrical models exist. Figure 6 illustrates an example employing CT and invasive contact mapping data to define the ablation target. Importantly, a concerning lack of reproducibility for target volume definition was found with up to 14-fold volume differences in clinical target volume between identical cases when assessed by five different university centres.56 Several prospective trials are currently ongoing, which will hopefully better inform and refine the SABR workflow to improve the safety and long-term efficacy of this modality.
Figure 6: Stereotactic ablative radiotherapy preprocedural planning steps
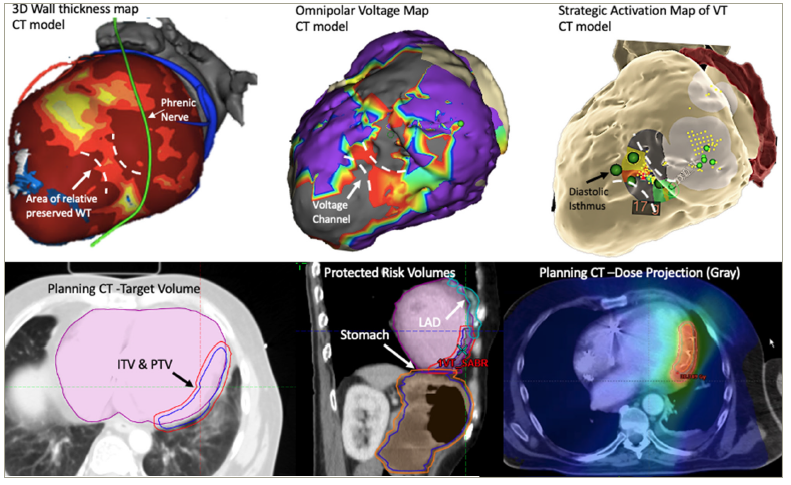
Top row: Noninvasive computerized tomography wall thickness map with a channel of relatively preserved wall thickness within an otherwise thinned out inferolateral wall. A contact map showed a low voltage channel at the same site (adjacent areas with erroneously high voltage due to far field signal annotation of the mapping system) and diastolic potentials during strategic ventricular tachycardia activation map during pulseless ventricular tachycardia. Procedure prematurely abandoned despite persistent clinical ventricular tachycardia due to hemodynamic deterioration. Bottom row: Based on computerized tomography and electroanatomical mapping system findings, a planned target volume was delineated onto axial computerized tomography and calculation of protected risk volume of adjacent structures including left anterior descending artery and stomach. Dose projection (colour coded according to grey) onto an exemplary axial computerized tomography slice is shown.
CT = computerized tomography; ITV = internal target volume; LAD = left anterior descending artery; PTV = planning target volume; SABR = stereotactic ablative radiotherapy; VT = ventricular tachycardia; WT = wall thickness.
Ventricular tachycardia substrate to target with stereotactic ablative radiotherapy
While noninvasive ablation would be an attractive choice for every patient (if long-term efficacy can be achieved and safety confirmed), the minimal periprocedural morbidity for undergoing SABR makes it particularly suitable for patients with VT with prohibitive risk and/or are too unstable to undergo conventional ablations, including patients with electrical storm.57 Furthermore, the option to precisely target nearly any given site in the heart, irrespectively of anatomical constraints, would allow to treat deep intramural or subepicardial substrates in patients with otherwise inaccessible pericardial space.
Chemical ventricular tachycardia ablation: Transarterial and transvenous Coronary Ethanol
Rational
Injection of high percentage (96 or 98%) ethanol into the myocardium has been suggested to achieve a chemical ablation via its cytotoxic protein denaturation effect.58 Intramural mapping over guide wires or small 2Fr linear mapping catheters can identify substrates deep within the myocardial wall, in close proximity to coronary arteries or otherwise inaccessible areas (e.g. due to severe pericardial adhesions or postcardiac surgery precluding epicardial access etc.) and subsequently targeted by the delivery of ethanol.
Evidence
Two main approaches for ethanol ablation to treat VAs have been proposed: transarterial coronary ethanol ablation and retrograde coronary venous ethanol ablation.59 The latter has been developed in an attempt to minimize the inherent risk of transarterial coronary ethanol ablation to cause coronary artery injury, thrombosis, dissection and risk of iatrogenic myocardial infarction.58,60 Detailed description of the procedural workflow for septal and nonseptal targets using the retrograde approach have been published.61 If access and cannulation of small branches are challenging and not suitable for standard single vein–single balloon ablation, advanced techniques have been proposed to reach the target zone (double balloon at distal and proximal part, using balloons in two different veins, intramural vein-to-vein cannulation with proximal balloon block or intramural ethanol).62
Over recent years, a number of case and series reports have demonstrated feasibility and evidence for the efficacy and safety of ethanol ablation for VAs.63–69 Data from a multicentre international registry for long-term efficacy and outcomes of retrograde coronary venous ethanol ablation included 56 patients (76% septal left ventricle, 24% nonseptal left ventricle), and reported a high acute success rate in 98% and 77% of patients were free of VAs at 12 months. The safety profile was equally as good with only two venous dissections leading to pericardial effusions described.70
Ventricular tachycardia substrate to target with ethanol
The classical target for ethanol ablations are deep septal and/or left lateral wall VT supplied by appropriate coronary venous or arterial branches (Figure 7).71 The obvious major limitation to any ethanol-related procedure is the dependency on suitable perforator branches to the target zone, whether it is arterial or venous. Furthermore, ethanol ablation depends on achieving high tissue concentration to achieve cytotoxic effect, though flow rate, vessel size and collaterals may affect the ultimate result, and final lesion size and homogeneity are only poorly controlled by the operator.
Figure 7: Ethanol ablation
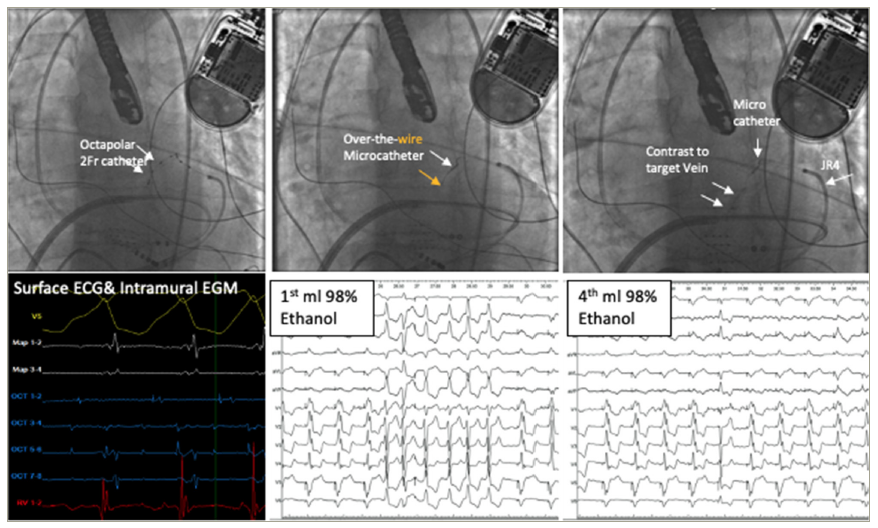
Top: Fluoroscopic images of insertion of 2Fr octapolar catheter into anterior interventricular vein, subsequent exchange for over-the-wire microcatheter and contrast injection. After identification of the target branch either a balloon-over-the-wire or, in small tortuous vessels, a direct approach by wedging a microcatheter can be employed. Careful assessment of collateral vein shunting via contrast injection is required. Prior to ethanol delivery, injection of iced saline may serve as a test run to gauge the effect of ablation at the intended ablation site (e.g. to assess for atrioventricular block). Typically, 1 ml of 96–98% ethanol is injected. Repeated injection of up to 4 ml in total over 2 minutes each may be performed to consolidate the effect and to overcome competing anterograde arterial flow. Capillary disruption following ethanol ablation has been described and has been associated with possible greater myocardial reach and thus improve ablative effects of repeated injections.71 Bottom row: Intracardiac EGMs during VT as recorded over octapolar catheter placed in coronary veins confirming mid-diastolic potentials intramurally. Surface ECG during ethanol injection to target sites shows flurry of clinical VT during first injection and no further reaction at time of 4th injection (1ml at each injection). (ECG and EGM image courtesy of Dr John Silberbauer, Royal Sussex County Hospital Brighton, UK)
ECG = electrocardiography; EGM = electrogram; JR4 = Judkins right coronary catheter.
Autonomous nervous system modulation
Antiadrenergic neuromodulation
Rational
The elevated risk of lethal VAs in the context of increased sympathetic or reduced vagal activity has been best characterized in the context of ischaemic heart disease, where sympathetic denervation is heterogeneous due to the post-infarct remodelling, sympathetic hypersensitivity and nerve sprouting in the border zone.72 The heterogenous decrease in action potential duration and increase in spatial dispersion of repolarization following sympathetic activation predisposes to VAs.73,74 In nonischaemic heart failure, sympathetic hyperactivity has equally been associated with VAs and the prognostic benefit of beta blockers has been partially traced back to their antiadrenergic effect.75 Lastly, sympathetic arousal is also a well-described trigger for VAs in catecholaminergic polymorphic VT, as well as certain subtypes of long QT syndrome (LQTS). Antiadrenergic neuromodulation techniques, notably cardiac sympathetic denervation. (Figure 8)76 have shown to be effective in reducing shock and VTs in these populations.
Figure 8: Antiadrenergic neuromodulation options
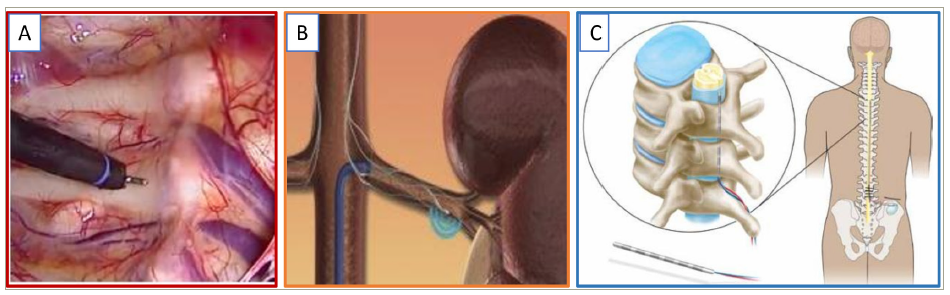
A. Thoracoscopic sympathectomy: Open thoracotomy approaches have mostly been replaced by minimal invasive video-assisted thoracoscopic techniques. Following exposure of the thoracic ganglia outside the pleura, the thoracic sympathetic chain is dissected. The image shows thoracoscopic view of sympathetic chain covered by (still intact) pleura. B. Renal sympathetic denervation can be achieved with commercialized percutaneous catheter ablation systems (reprinted with the permission of Medtronic, Minneapolis, MN, USA). C. Spinal cord stimulation: Example of percutaneous “needle” stimulator in epidural space and connection to a generator at the lower back/buttocks (reproduced from Harned et al.76 and reprinted with permission of the author).
Methods and evidence
Renal sympathetic denervation
Percutaneous ablation of the renal autonomic nervous connections may reduce afferent sympathetic input to the central nervous system as well as reducing effect signalling to the renal parenchyma, and thereby reduction of the renin angiotensin aldosterone system activation. Direct antiarrhythmic effects may be due to structural and electrical remodelling including decrease in sympathetic nerve sprouting.77 Renal denervation for treatment of VAs showed encouraging results in various small case series of patients with structural heart disease with refractory arrhythmias,78–80 patients with chronic kidney disease and VAs,81 and in isolated case reports for catecholaminergic polymorphic VT (CPVT) and LQTS.82,83
Spinal cord stimulation
Spinal cord stimulation (SCS) reduces sympathetic tone, suppresses activity generated by intrinsic afferent sensory cardiac neurons related to sympathetic excitation and the excitatory effects on the neural ends by local diseased myocardium (e.g. during ischaemia).84 Equally, SCS may enhance vagal tone and prolong the ventricular refractory period.85 In animal studies, acute and chronic spinal cord stimulation was associated with a reduction in VAs and improved ventricular function in models of myocardial infarction and pacing induced heart failure with objective suppression of the simultaneously recorded left stellate ganglion activity.86,87 In an ischaemia reperfusion model, SCS reduced VAs and was associated with a stabilization in repolarization abnormalities.88 A human feasibility trial for SCS in VAs, between 2007 and 2011, was prematurely stopped due to lack of patient recruitment.89 Only two patients were enrolled for whom a significant reduction in VAs post-SCS implantation and stimulation at the T3 level was documented.
Surgical cardiac sympathetic denervation
Beyond the well known antiadrenergic effects, a reflex increase in cardiac parasympathetic activity, antagonism of neuronal remodelling and correction of imbalance in the neurotransmitter system appear to also play a role in the antiarrhythmic effect of cardiac sympathetic denervation.90 It has been shown to reduce VAs, cardiac events and implantable cardioverter/defibrillator shocks in a number of studies for patients with LQTS,91–94 CPVT95,96 and structural heart disease with drug-refractory electrical storm.97,98 In patients with structural heart disease, worse outcomes with left sided-only cardiac sympathetic denervation, VTs with longer cycle length and advanced New York Heart Association status have been reported.99
Percutaneous pharmacological stellate ganglion blockade
Percutaneous application of local anaesthetics, particularly if applied as continuous infusion, has been demonstrated to be an effective adjunctive strategy to attenuate VAs in the context of electrical storm.100 Within 24 hours, patients were free of VA and had a lower hospital mortality than patients with continued VA.101
Investigational
Chemogenetics is an investigational approach using ‘designer receptors’ that are introduced to the target cell (cardiomyocyte or neuron) to change cell activity. In optogenetics, light sensitive proteins are employed in a similar manner and can be controlled by photo stimulation. Precise, tailored modulation of the peripheral or central autonomic nervous system and signalling pathways may therefore become feasible. A combination with wireless technology has already been proposed and tested in animal studies.102 The feasibility of remote stellate ganglion neuromodulation via subcutaneous implantation of wireless transmitter has been reported.103
Vagal stimulation
Rational
Enhanced vagal tone promotes ventricular electrical stability in patients with acute ischaemia and previous myocardial infarction. Mechanistically, the cardiac effects of vagus nerve stimulation are thought to be mediated by suppression of the ganglionated plexi activity (demonstrated by marked suppression of frequency and amplitude of the neural activity within the ganglionated plexi)104 of both the adrenergic and cholinergic components, and the stellate ganglion nerve activity.105–107 Furthermore, a beneficial impact on ventricular remodelling and an anti-inflammatory effect, which in turn may contribute indirectly to arrhythmia suppression, has been suggested. Examples of vagal nerve stimulation are illustrated in Figure 9.108
Figure 9: Examples of interventional vagus stimulation
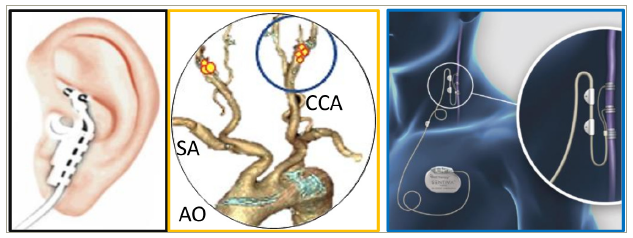
A. Noninvasive auricular branch vagus nerve stimulation with ear clip, here shown as attached to conchae cymba (reproduced from Dumoulin et al.108 and reprinted with permission of the author) B. Computerized tomography aortogram with schematic representation of location of carotis sinus with baroreceptors. Stimulation at this site activates the glossopharyngeal nerve and elicits the baroreceptor reflex with an increase in parasympathetic activity. C. Invasive low-level vagus nerve stimulation over commercially available implantable leads with infraclavicular generator position (reprinted with permission of LivaNova, PLC, London, UK)
Methods and evidence
Low-level vagus nerve stimulation
Low-level vagus nerve stimulation is traditionally delivered via a small surgical procedure to the right (for cardiac indications) or the left (more commonly for noncardiac indications) cervical segment of the vagus nerve with the neurostimulator generator positioned in the prepectoral area to stimulate the vagus nerve.109 A noninvasive handheld device for self-administration achieving vagus nerve stimulation via stimulation through the skin has been approved.110 Evidence of successful suppression of VAs is limited to animal studies of acute ischaemia and chronic post-infarct.111,112
Auricular branch-vagus nerve stimulation/low-level tragus stimulation
The transcutaneous stimulation of the auricular branch of the vagus nerve can be achieved via an ear clip attached to the tragus, though optimal stimulation protocols remain under debate. In animal models, attenuation of negative structural remodelling and inflammation, and decreased cardiac sympathetic nerve sprouting and suppression of VAs with a flattening of the restitution curve slope has been described as an underlying antiarrhythmic mechanism.113 A randomized, sham-controlled proof-of-concept trial in patients with myocardial infarction showed a decrease in VAs within 24 hours of the index event, and biomarkers of myocardial injury and inflammation.114
Baroreflex activation therapy
VAs have been associated with a depression in the baroreflex sensitivity.115 Commercialized baroreflex activation therapy systems use a surgically implanted carotid sinus lead and a pulse generator, which is implanted subcutaneously in an infraclavicular chest wall pocket.116 Activation of the baroreceptors in the carotis sinus increases parasympathetic activity and causes a reflex reduction in sympathetic nerve activity. In the ventricle, this has been associated with stabilization of the ventricular electrophysiological properties and prolongation of effective refractory period, and reduced incidence of ventricular tachycardia/fibrillation in animal infarct models.117 Baroreflex activation therapy has been successfully employed in the treatment of heart failure; however, no dedicated studies for VT have been published.118,119
Hybrid and stand-alone ventricular tachycardia surgery
For patients with refractory VT and/or inaccessible substrate despite any of the before-mentioned percutaneous or noninvasive approaches, collaboration with cardiac surgeons to perform hybrid procedures (surgical access and conventional electrophysiological mapping/ablation) or stand-alone surgical ablation remains a valuable management option. The procedural approach depends on the suspected critical area and target zones.120 A subxiphoidal window allows access to the inferior and inferolateral left ventricular substrate; whereas, a limited anterior or anterolateral thoracotomy or video-assisted thoracoscopy can target the lateral, apical and anterior wall.121,122 A median sternotomy should be reserved for patients requiring concomitant cardiac surgery or if previous approaches have failed. Pure surgical VT treatments, by means of aneurysmectomy and subendocardial resection, are rarely performed in current practice.
Conclusions
The spectrum of available treatment modalities for VT is rapidly increasing, offering opportunities and challenges. Ethanol ablation, ultra-low temperature cryoablation and pulsed field modalities appear as the most promising technologies and strategies to complement existing radiofrequency approaches for VT ablation in the near future. In turn, laser/photoablation and acoustic wave modalities remain purely investigational and despite intriguing concepts and preclinical data, are unlikely to be implemented in our clinical routine any time soon.
Noninvasive stereotactic radiotherapy appears to be the most desirable solution in the commonly multimorbid VT population if the efficacy and safety for this purpose can be unequivocally confirmed. Yet, its use in cardiology is still in its infancy with a number of important practical questions requiring answers prior to it being considered outside of clinical trials. Imaging guided noninvasive-HIFU may be an even more desirable noninvasive VT ablation approach without the need of ionizing radiation, though its feasibility in humans has not yet been established, let alone safety and efficacy.
Neuromodulation has rightfully gained a lot of momentum in recent years after having been a long neglected component to be addressed in clinical VT management. Cardiac sympathetic denervation is increasingly performed for LQTS and CPVT, but also structural VTs, and is an important complementary therapeutic option. However, in general the lack of reliable and accurate assessment of the autonomic activity in humans and its dynamic and transient impact on the cardiac substrate remain a major barrier preventing a more refined patient selection, choice of modality and titration of neuromodulation.
With growing experience, more widespread use and improvement in the presented techniques and equipment, each of the methods will likely have a valued place in the armamentarium of clinical electrophysiologists. Given the complexity of ventricular arrhythmogenesis, any ablation strategy, regardless of the energy source employed, will need to be tailored to the patient’s characteristics and address the different structural, electrical and autonomic factors contributing to the VT in order to improve patient outcomes and arrhythmia-free survival.
