Background: Conduction system pacing has the potential to offer improved outcomes compared with other forms of pacing. His bundle pacing (HBP) can be technically more difficult to achieve and pacing thresholds can be unreliable compared with left bundle branch area pacing (LBBAP). There are no reports describing the feasibility of performing both procedures in the same patient and here we present a unique case report demonstrating its feasibility, as a proof of concept and highlight some important learning points.
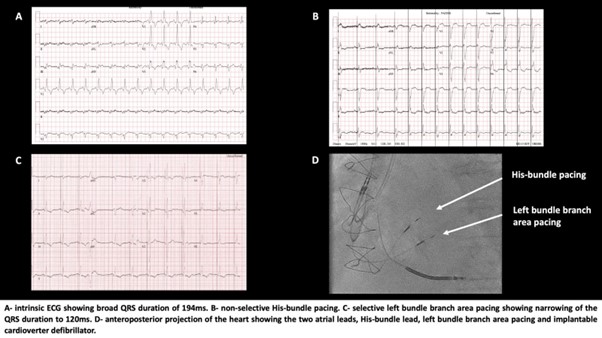
Case: A 67-year-old patient with a history of ischaemic heart disease, coronary artery bypass grafting and mitral valve replacement was referred for primary prevention implantable cardioverter defibrillator. He had first-degree heart block of 230 ms with a QRS duration of 122 ms and severe left ventricular systolic impairment 26%. It was felt that he may require pacing, and after discussing at the multi-disciplinary meeting, he underwent HBP with an atrial lead and implantable cardioverter defibrillator as part of the HOPE-HF trial. The procedure resulted in non-selective His capture, with a threshold of 2.2 Mv at 1 ms. Following implantation, he felt less breathless, but his left ventricular systolic function remained similar at 29%. Four years later, he had episodes of paroxysmal atrial tachycardia with a rapid ventricular response and rate control was proving to be difficult. In addition, his His-bundle threshold increased to 3.5 Mv at 1 ms and a generator replacement was required due to premature battery depletion. He now had broad right bundle branch block of 194 ms and a venogram showed an occluded left subclavian vein. His case was discussed at the multi-disciplinary team meeting at length and given his multiple co-morbidities it was felt transvenous lead extraction was too high risk and he no longer needed an ICD due to his poor prognosis. Given the difficulty with rate control, the consensus was to attempt LBBAP from the right side resulting in more physiological activation with a narrower QRS duration, abandon the left-sided implant and then undergo an atrioventricular nodal ablation in future. A Medtronic 3830 lead was implanted and LBBAP was achieved using previously defined criteria; right bundle branch morphology and a constant V6 peak left ventricular activation time of <80 ms at 5 V and 1 V or transition from non-selective to selective left bundle branch capture at near-threshold outputs. The sensing was 20 Mv, threshold 0.5 V at 0.4 ms and final paced QRS duration was significantly lower at 120 ms. There were no acute complications and the patient improved symptomatically.
Conclusion: Conduction system pacing has many advantages and may become the predominant form of pacing. We have demonstrated that LBBAP is possible in a patient with HBP and this led to greater physiological activation. Although LBBAP is technically easier than HBP, implantation from the right side was more challenging requiring greater guide support to be successful. ❑
Figure 1