Introduction: There is limited experience of ultrasound (US) guided axillary vein access for cardiac electronic device implantation in the United Kingdom. We investigated the safety, efficacy, learning curve, and radiation exposure of US-guided axillary vein access.
Methods: US-guided axillary vein access was attempted in consecutive patients requiring cardiac device implantation between June 2018 and November 2019. Procedures were performed by an experienced electrophysiologist with no prior application of the technique. Access (needle to wire) and fluoroscopy times for US-guided access were compared to times for conventional fluoroscopy landmark-guided access in ten consecutively acquired control patients.
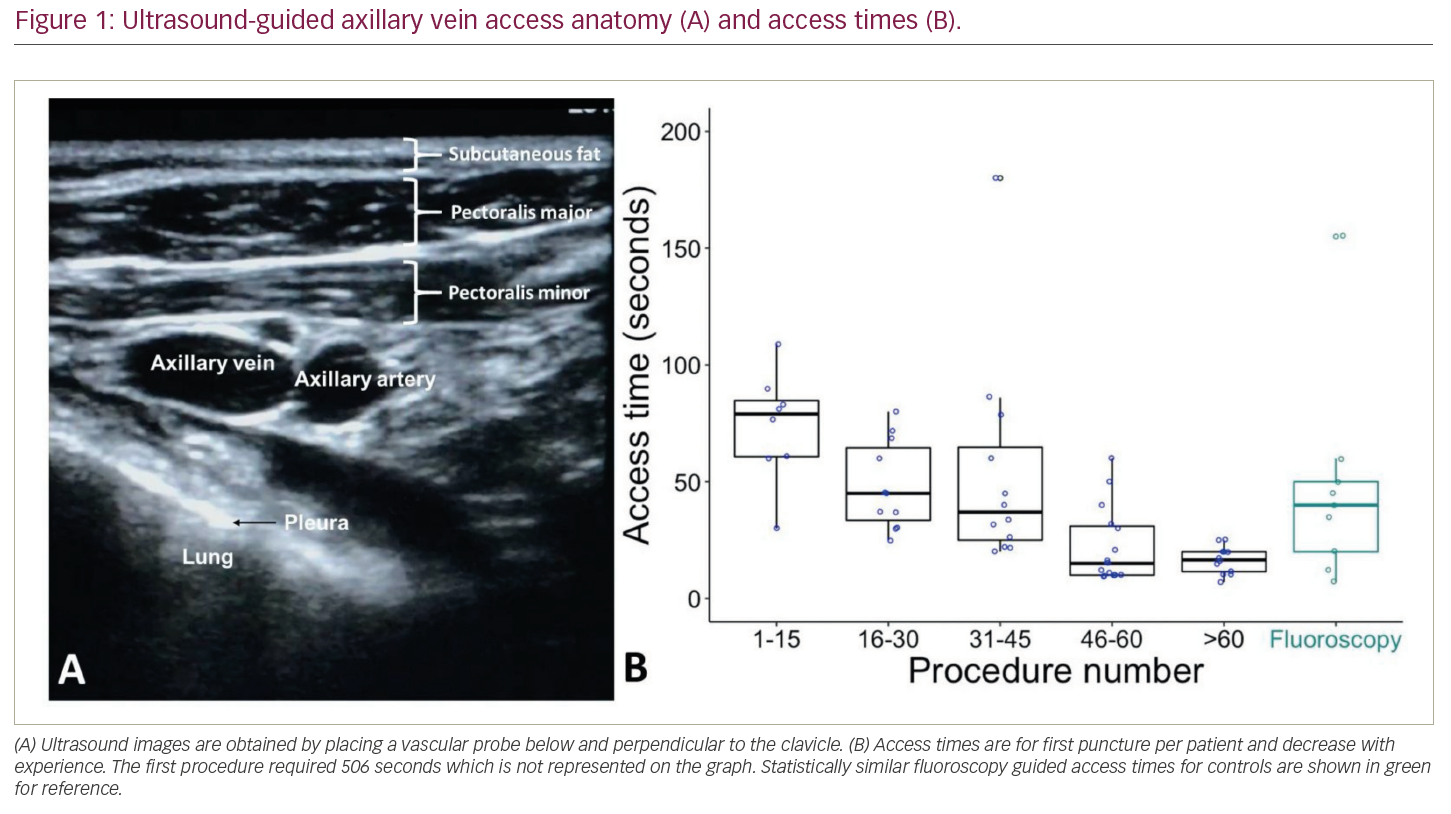
Results: US-guided axillary vein puncture was successful in 72 (97%) of 74 patients attempted (age 72 ± 16 years, 58% male), who required 147 punctures for one (8%), two (71%) or three (17%) leads, or upgrades (4%). In the two patients with unsuccessful US-guided access, the axillary vein was either not visualized (small calibre on subsequent venography) or situated deeply with prohibitively steep wire angulation. There were no peri-procedural complications related to venous access, including pneumothorax. US-guided access time ranged from 5 to 506 seconds per puncture. First US-guided puncture per patient was 30 (interquartile range, IQR: 17,60) seconds, and was similar to fluoroscopy guided access time (43, IQR: 24,58 seconds; p=0.45). Time for US-guided access decreased from 81 (IQR: 61,90) to 16 (IQR: 10,20) seconds from the first to the last fifteen procedures (p<0.001). 69 (96%) patients did not require fluoroscopy using US-guided access. 3 (4%) patients required 1 second fluoroscopy time after successful US-guided access to confirm 0.035-inch J wire position due to difficult passage. Controls required 29 (IQR: 17,56) seconds of fluoroscopy time for access, resulting in 0.25 (IQR: 0,1.4) mGy cumulative skin dose, and 0.03 (IQR 0.02–0.5) Gy.cm2 effective dose area product, and equivalent to 0.64 (95% confidence interval: 0.16–1.45) chest radiograph radiation exposure.
Discussion: Ultrasound guided axillary venous access for cardiac device implantation is a feasible alternative to fluoroscopy guided access, and reduces radiation exposure. The learning curve time is acceptable, and the procedure is safe, even during training.