Lead displacement in pacemakers is a common implantation-related procedural complication, often resulting in prolonged hospital stays for patients and increased healthcare costs.1,2 The frequency of long-term lead displacement ranges between 1.8% and 8.0%.3,4 Recognizing lead displacement complications is an essential part of caring for patients with these cardiac devices.1
Case report
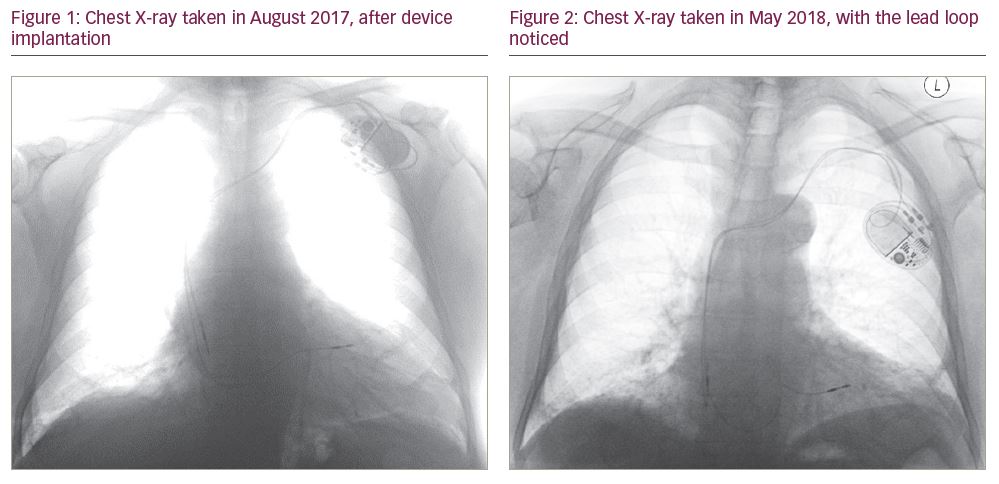
An 89-year-old man underwent implantation of a dual-chamber pacemaker in August 2017 for sinus node dysfunction (Dual chamber Abbott/St Jude Assurity – MRI 2272 pacemaker), with bipolar Abbott/St Jude leads 2088TC 58 cm and 52 cm [all Abbott Laboratories, Chicago, IL, USA]), with no acute complications. The right ventricular (RV) lead was implanted in a septal position, with an implant threshold of 1.9 V at a pulse duration of 0.4 msec. The post-procedural chest X-ray can be seen in Figure 1.
During a routine pacemaker follow-up in May 2018, it was noted that the RV threshold had increased to 3.9 V at a 0.4 ms pulse duration. RV lead impedance was stable and RV bipolar sensing was measured at 7.2 mV.
A repeat chest X-ray was performed, which showed no displacement of the RV lead tip, but revealed a loop of RV lead in the RV outflow tract that was not present on the previous chest X-ray (Figure 2). The position of the atrial lead was unchanged. As the RV pacing burden was very low (<5%), it was decided not to reposition the RV lead at that stage, but to continue monitoring the RV lead threshold.
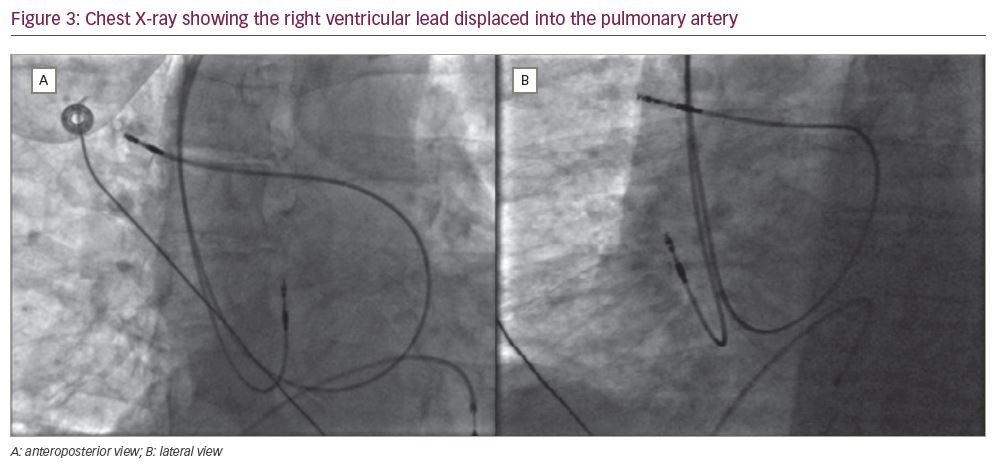
In June 2019, persistent noise was noted on the RV lead. The RV lead threshold was 7.25 V @ 1.0 ms bipolar and 1.0 V @ 0.4 ms unipolar. The RV pacing was reprogrammed to unipolar, with RV bipolar sensing measured at 4.5 mV. The patient was asymptomatic; however, he was scheduled for RV lead revision. Prior to opening the pacemaker, fluoroscopy of the leads pocket demonstrated that the RV lead had been displaced, with the lead tip now located within the right pulmonary artery (Figure 3). The lead was extracted with simple traction and a new RV lead was implanted at the RV apex.
Discussion
Here we present the case of a patient in whom the RV pacemaker lead migrated to the pulmonary artery due to progressive slack in the lead over time. We refer to this case as an example of ‘reverse ratchet’ syndrome. Serial chest X-rays showed advancement of lead slack into the central circulation, with eventual displacement of the RV lead. It is noted that the pacemaker orientation changes before eventual displacement of the lead into the RV outflow tract, and then into the pulmonary artery. The lead slack advanced due to a loose lead fixation (suturing) sleeve, arm movements and anticlockwise rotation of the pacemaker. The combination of these factors resulted in this reverse ratchet syndrome.
Twiddler’s syndrome and reel syndrome have been described as the retraction and displacement of the lead due to the rotation of the device battery around the long axis and the horizontal axis.5,6 Twiddler’s syndrome is conscious or unconscious manipulation of the pulse generator, causing it to rotate around its long axis.5 Reel syndrome occurs due to the rotation around the short axis of the battery.6
Ratchet syndrome has a different mechanism from Twiddler’s and reel syndromes. In the case of ratchet syndrome, the lead progressively retracts from the implantation vein due to arm movement and an improperly tied lead fixation sleeve.7 In the case we have described, the patient rotated the generator on its transverse axis, rolling the lead around the generator and provoking lead displacement. Chest radiography is crucial to diagnose this kind of complication.6 In the case of Twiddler’s syndrome, when the device pocket is reopened, the lead is observed to be twisted around itself in a spiral-shaped fashion. However, in reel and ratchet syndromes, the lead is observed to be circled around the device. Thus, it can be difficult to distinguish between reel and ratchet syndromes simply based on the condition of the lead in the pocket.8
Summary
In the case we have presented, the patient did not show any symptoms relating to pacemaker lead displacement. Lead slack progressed over a long period, and displacement was seen relatively late. The pacemaker had rotated anticlockwise with the lead slack causing a loop in the RV lead in the RV outflow tract, which eventually led to the retraction of the RV lead tip from the RV implantation position and displacement into the pulmonary artery.
Patient education about post-pacemaker implant care, creating an appropriately-sized pocket for the generator, tying the lead fixation sleeves so they are sufficiently tight and fixing the battery to the pocket tissue with a strong suture can be used to avoid lead displacement, a well-known complication of device implantation.1,2