Background: The presence of a spontaneous type 1 Brugada ECG pattern and previous syncope or cardiac arrest have consistently been associated with increased risk of sudden cardiac death (SCD) in Brugada Syndrome (BrS). In contrast asymptomatic individuals with a drug-induced type 1 pattern are at low risk. However, the ECG phenotype is known to be highly dynamic. We hypothesised ambulatory 12-lead ECG may be superior to ajmaline provocation for identifying patients with BrS and a moderate-to-high risk of arrhythmic events.
Methods: Patients with a previously documented type 1 Brugada ECG pattern (spontaneous, fever- or ajmaline-induced) underwent 12-lead 24-hour ambulatory ECG monitoring with modified high RV leads. Patients were classified as either ‘≥ Moderate Risk (previous spontaneous type 1 ECG pattern or previous arrhythmic syncope/cardiac arrest) or ‘Low Risk’ (Asymptomatic and a drug-induced ECG pattern only). The presence of Brugada ECG patterns and J-point amplitude (irrespective of ECG morphology) were recorded at 30 min intervals throughout 24 hours. The 24-hour ‘Type 1 burden’ was calculated as time present (hours) x number of leads present). Findings in ≥ Moderate Risk and Low Risk groups were compared.
Results: The cohort comprises 18 patients (78% probands, 72% male, mean age 39 ± 14 years). There were 7 (39%) patients classified as ≥ Moderate Risk and 11 (61%) as Low Risk. Prior spontaneous type 1 ECG was present in 6 (33%). Two patients had prior aborted cardiac arrest. An intermittent type 1 ECG was seen for ≥1 hour in 5 (28%) patients.
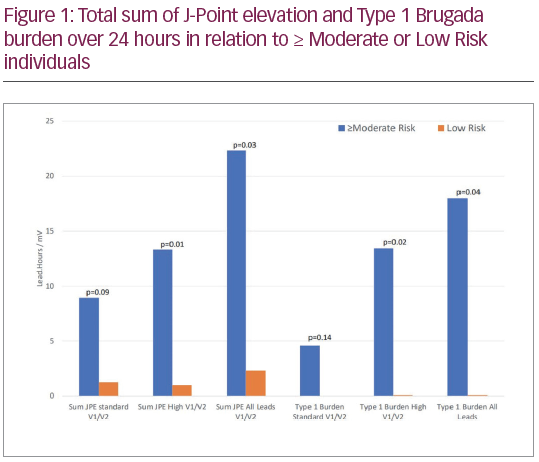
≥ Moderate Risk patients displayed a higher ‘type 1 burden’ in standard and high RV leads (18.0 ± 26.7 versus 0.1 ± 0.3 lead.hours, p=0.04) and sum J-point elevation over 24 hours (22.3 ± 27.6 versus 2.3 ± 3.3 mV, p=0.03) than low risk patients (see Figure 1). Prospective data collection and analysis is ongoing.
Conclusions: Ambulatory 12-lead ECG differentiates low risk from
≥ Moderate Risk patients and may be superior to ajmaline provocation in identifying patients with prognostically significant BrS. Sum J-point elevation over 24 hours may represent a novel risk marker for arrhythmic events in BrS.