Background: Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a rare, inherited non-ischaemic cardiomyopathy, which is linked to a high incidence of recurrent ventricular arrhythmias (VA) and sudden death, especially in young and athletic people. The purpose of this study was to describe the experience with mexiletine and sotalol combination for the treatment of VA.
Methods: This was a single-centre, observational cohort of patients with ARVC seen at the Inherited Cardiac Condition Services at University Hospitals Birmingham (UHB) between 2010 and 2022. ARVC patients being treated with mexiletine and sotalol were identified by digital health records. Electrocardiographic, imaging, device and genetic testing data were analysed in this cohort. The type of VA and the treatment with antiarrhythmic therapy in relation to defibrillator implantation and ablation were examined.
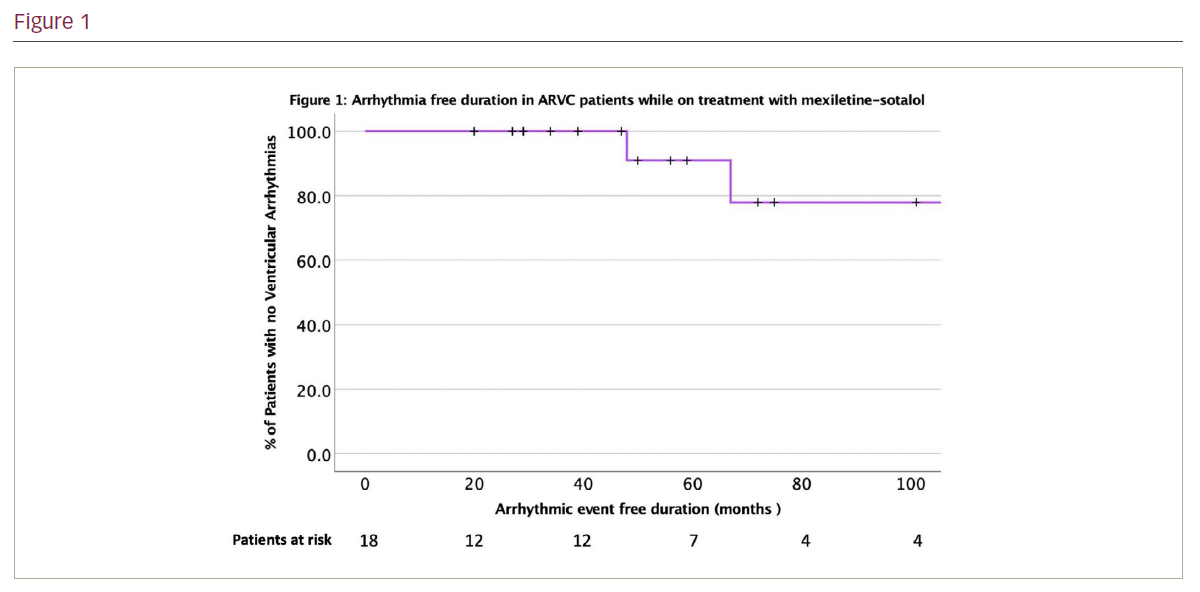
Results: A total of 18 patients (mean age 45 ± 12 years, 72% male) were on treatment with mexiletine and sotalol combination out of a cohort of 165 patients with definite, borderline and possible ARVC. All 18 met diagnostic 2010 Task Force Criteria for ARVC. A total of 13 patients had documented sustained ventricular tachycardia, while four patients had high burden ventricular ectopy and one patient had a ventricular fibrillation arrest. An implantable cardioverter defibrillator was implanted in 13 patients, and 5 patients underwent catheter ablation (3 patients had endocardial while 2 patients had combined endocardial-epicardial ablations) for VA. Epsilon waves were identified on 12-lead electrocardiogram (ECG) in 6 patients (33%) while late potentials were found in signal averaged ECG (SAECG) in 11 patients (61%). Left ventricular (LV) ejection fraction was 55 ± 12%, while right ventricular (RV) fractional area change (FAC) was 29 ± 9%. Late gadolinium enhancement (LGE) of the ventricular myocardium was identified in 11 patients (10 had RV LGE and 5 had LV LGE). Plakophilin-2 (PKP2) was the most identified genetic mutation (11 patients, 56%). Participation in sports was reported by 11 patients (61%). The mean dose of mexiletine was 558 mg per day (range 300–900 mg/day) while the mean dose of sotalol was 149 mg/day (range 80–360 mg/day). Arrhythmic event-free duration on the mexiletine-sotalol combination in these patients was found to be 61 ± 32 months during follow-up (Figure 1).
Conclusion: VA is an important cause of morbidity and mortality in patients with ARVC. Mexiletine-sotalol combination is a useful adjunct to ablation and defibrillator implantation in these patients and provides effective arrhythmia-free periods in these high-risk patients. Larger datasets are required to compare the efficacy of the mexiletine-sotalol combination with other antiarrhythmic drugs in patients with ARVC. ❑