Introduction: Wolff–Parkinson–White (WPW) syndrome is an important cause of arrhythmias in children. Despite having significant evidence and guidelines on diagnosis and management of this condition, it still proves enigmatic. We discuss here three cases with late manifestations of WPW syndrome that were not evident on previous electrocardiograms (ECGs), Holter and exercise tests.
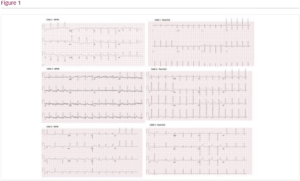
Case 1: A 14-year-old girl with previous patent ductus arteriosus (PDA) Amplatzer device closure had presented with recurrent episodes of dizziness, light headedness and easy fatigue during exercise. She was previously well with normal ECG and exercise test. Repeat ECG this time, however, showed bradycardia (heart rate 56 bpm) with short PR interval of 80 ms, overt pre-excitation and wide QRS (146 ms). Echocardiogram showed reduced left ventricular function with fractional shortening (FS) 21%. Incremental atrial and ventricular pacing mapped an accessory pathway at the 7 o’clock position at tricuspid annulus, which was then successfully ablated. Post-procedure ECG showed sinus rhythm and the echocardiogram showed improved ventricular function (FS 35%).
Case 2: A 23-year-old woman who was under regular cardiac surveillance since the age of 2 in view of strong family history of hypertrophic cardiomyopathy presented with palpitations. All through her surveillance, her ECG, echocardiogram, 24-hour Holter (twice) and cardiac magnetic resonance imaging (at age 21 years) were normal. However, a repeat ECG at the emergency department showed a narrow complex tachycardia associated with ectopics and suspected pre-excitation at age 23. Electrophysiology (EP) study demonstrated a bidirectional accessory pathway conduction at the 6 o’clock position on the atrioventricular groove with a life-threatening behaviour following isoprenaline (antegrade effective refractory period [ERP] <220 ms; retrograde ERP 240 ms). A successful ablation was performed. Post-procedural ECG showed normal sinus rhythm with no pre-excitation.
Case 3: A 13-year-old girl with a past history of spontaneously closed muscular ventricular septal defect (VSD) at 2 years of age presented with recurrent episodes of shortness of breath and chest tightness. Her previous ECG during VSD surveillance was normal, as was her echocardiogram. Repeat ECG during initial presentations of chest tightness showed occasional ectopics, but otherwise normal findings. Hence, a Holter was arranged. However, she presented 1 week later with worsening symptoms and ECG managed to capture delta waves with short PR interval (98 ms) and widened QRS (140 ms). Interestingly, her repeat ECG 24 hours later was normal again. She was thus started on flecainide and is currently awaiting EP study.
Conclusion: We have here three girls who were under intensive cardiac surveillance for various reasons and have had documented normal ECG findings with no evidence of delta wave previously. All three presented again in teenage or young adult age with varying symptoms and were found to have WPW syndrome. This highlights the importance of concealed and late-presenting WPW and the challenges in its diagnosis on not only spot ECGs, but also Holter and exercise tests. Further re-evaluation of existing diagnostic guidelines for excluding WPW may be necessary to identify these patients, including the use of wearable ECG devices and regular follow-up despite normal ECG.