Background: Cardiac magnetic resonance (CMR) with late gadolinium enhancement (LGE) imaging can detect subtle abnormalities including scar undetectable by echocardiography, and hence may aid diagnosis and guide clinical management in patients with premature ventricular contractions (PVCs) where decision making can be complex. However, it remains unclear which patients are most likely to benefit from further CMR assessment.
Objective: To determine clinical and electrocardiographic predictors of LGE on CMR in patients with PVCs and normal echocardiogram, and the subsequent impact on clinical management.
Methods: Consecutive patients referred for CMR for PVC assessment (1,000/24 h or 1% burden) with normal baseline echocardiograms between 2015 and 2020 were included. CMR parameters were analysed using artificial intelligence for standardization. Electrocardiograms (ECG) were analysed for PVC origin and clinical abnormalities. A total of 94 patients with PVC number of 1,000/24 h or 1% burden, and normal baseline echocardiograms were identified. Follow-up endpoints were: 1) whether CMR LGE findings resulted in a new cardiac diagnoses and/or change to clinical management; 2) death or significant arrhythmia requiring device implantation.
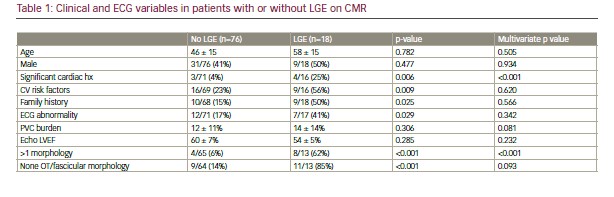
Results: A total of 94 patients (57% female, age 48 ± 16 years) were included with mean echocardiographic LV ejection fraction of 59 ± 7%, median PVC burden of 8% (interquartile range [IQR] 3–19%) and CMR LV ejection fraction of 61 ± 8%. LGE was detected in 18/94 (19%) scans. Predictors of LGE were: patients with significant previous cardiac history (previous coronary disease, myocarditis), conventional cardiovascular risk factors, family history, abnormal baseline ECG, more than 1 PVC morphology (polymorphic PVCs) and non-outflow tract/non-fascicular morphology were all more likely to have LGE on CMR (Table 1). Significant cardiac history and polymorphic PVCs were both independent predictors on multivariate analysis. At mean follow-up of 3 ± 1.6 years, 6/18 LGE vs 2/76 no LGE (33% vs 3%; p<0.001) patients had a new diagnosis resulting in initiation of medications and/or continued specialist follow-up. Two LGE patients required device implantation (permanent pacemaker [PPM] for advanced AV block with septal mid-wall LGE; ICD for arrhythmogenic right ventricular cardiomyopathy, with ring-like subepicardial LGE). In the non-LGE group, 1 had ICD for syncopal VT and new LGE detected at 3-year interval scan, and 1 died of metastatic pancreatic cancer at 4.9 years.
Conclusion: Older patients with normal echocardiograms but a significant cardiac history, polymorphic PVCs or non-outflow tract/fascicular origin, are likely to have focal scar on further assessment with CMR imaging. LGE detected on CMR aids diagnosis of cardiomyopathy although the long-term prognostic value remains to be determined. ❑