Introduction: A greater biventricular pacing percentage (BiVp%) is associated with greater left ventricular reverse remodelling and reduction in all-cause mortality in patients with cardiac synchronisation therapy devices (CRT). A multi-disciplinary team (MDT) service was implemented at Barts Health NHS Trust to discuss patients with low BiVp%, to determine the cause, increase BiVp%, and provide a clear management plan to aid cardiac scientists when responding to remote monitoring alerts.
Methods: This retrospective audit followed 121 patients who were referred to the low BiVp% service between June 2020 and July 2021. 106 patients were included in the analysis, of the excluded patients, 11 were deceased at 6 months, 3 had been transferred to another centre and one patient had left ventricular (LV) lead displacement. Baseline characteristics were collected at time of CRT implant and BiVp% and New York Heart Association (NYHA) functional class were collected at the time of MDT and 6-month post MDT. The outcome of the MDT was actioned and documented on patients’ electronic health records.
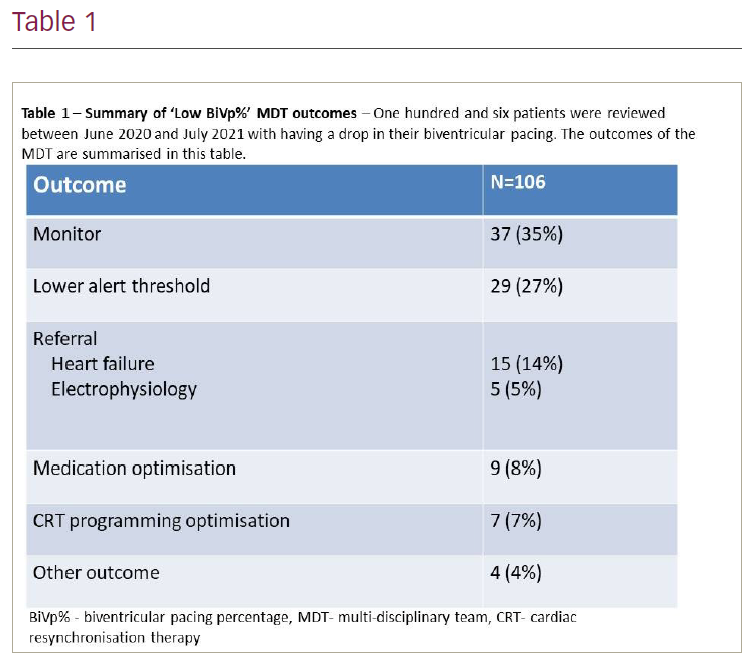
Results: Of the 106 patients, 75% were male, mean age was 73 ± 10.6 years, mean LV ejection fraction (LVEF) at implant was 33 ± 11% and 57% were classed as NYHA II. The most common indication for implant was ischaemic heart disease (49%), and the most common QRS morphology was left bundle branch block (58%). The most common outcomes were to continue patient monitoring (35%) and lowering the alert threshold on remote monitoring (27%). In the remaining 40 patients, an active outcome was actioned, most commonly a referral to another cardiology service (19%). The other outcomes are summarised in Table 1. These 40 patients had a mean improvement in BiVp% of 6 ± 12% over a mean follow-up time of 5.9 ± 1.6 months post-MDT. An improvement of ≥1 NYHA class was seen in 16 patients (44%), no change in NYHA class was seen for 12 (33%) symptomatic patients (NYHA II-IV), no change in NYHA class was seen in 6 (16%) asymptomatic patients (NYHA I) and 2 patients showed a worsening of ≤1 NYHA class at a mean follow-up time of 5.9 ± 1.6 months post-MDT.
Conclusion: This retrospective audit has demonstrated that in 38% of patients being discussed in a ‘low biventricular pacing MDT’, active changes were made to their clinical care. These patients had an improvement in biventricular pacing and around half had improved NYHA class over a short follow-up period. Changing alert threshold was a useful outcome for cardiac scientists when managing remote monitoring alerts. Future prospective studies should evaluate the outcomes over a longer follow-up duration. ❑