Background: Incidental LBBB (iLBBB) is a frequent cause for cardiology referrals. In such instances, there may be uncertainty as to its prognosis and need for clinical follow-up. Cardiovascular magnetic resonance (CMR) is the gold-standard for myocardial phenotyping.
Objectives: To determine the utility of CMR in the risk stratification of patients with iLBBB.
Methods: CMR was used to identify the myocardial phenotype of patients with iLBBB. We compared outcomes of patients with an iLBBB with (iLBBBCMR+) or without (iLBBBCMR–) an abnormal CMR scan with healthy controls as well as age- and sex-matched individuals in the general population (life tables).
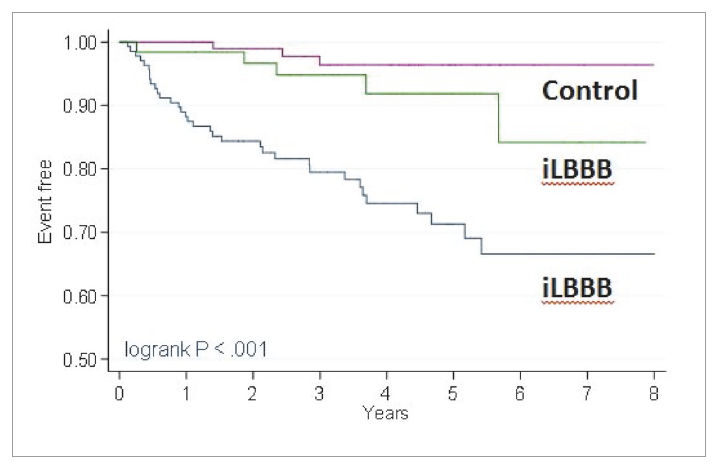
Results: In patients with iLBBB (n=199, aged 62.9 ± 12.6 years (mean ± SD), CMR was abnormal in 136 (68.4%) and was attributed to ischaemic (30 [15.1%]), non-ischaemic (94 [47.2%]) causes, hypertension (24 [12.1%]) and aortic valve disease (7 [3.5%]). Over 4 (2.5–5.3) years (median [interquartile range]), iLBBBCMR+ had a higher risk of total mortality or major adverse cardiac events (adjusted hazard ratio [aHR]: 8.48, 95% confidence interval [C.I.] 2.56–28.1, p<0.001), total mortality (aHR: 4.96, 95% C.I. 1.44–17.1, p=0.011) and total mortality or heart failure hospitalisation (aHR: 7.75, 95% C.I. 2.31–26.0, p=0.001) compared with controls. iLBBBCMR- had a similar risk of all endpoints. iLBBBCMR- patients had a similar survival to controls and the general population.
Conclusions: Over two thirds of patients with a iLBBB had an abnormal myocardial phenotype on CMR. Outcomes in iLBBBCMR+ were poor. Survival in iLBBBCMR- was comparable to the general population.